
'Norwegian Study: Corona Infection Linked to Hidden Heart Damage'
'A recent study based on data from the Trøndelag Health Survey (HUNT) shows that the virus also leaves invisible traces [orig. usynlige spor] in the general population.' ∽ NRK journo™ Jan-Erik Wilthil

A long posting to follow-up on yesterday’s reporting:
It looks like we’re in another couple of days of heavy Covid-related rah-portin™.
Translation, emphases, and [snark] mine.
Norwegian Study: Corona Infection Linked to Hidden Heart Damage
A new Norwegian study shows that Covid-19 is linked to an increased risk of imperceptible, chronic damage to the heart. The researchers have found a disturbing signal in the blood of thousands of Norwegians after the pandemic.

By Jan-Erik Wilthil, NRK.no, 7 June 2026 [source; archived]
Measurements show that the degree of heart damage may have increased after the pandemic. It seems that we can link it to Covid-19.
Thus Professor Torbjørn Omland from the University of Oslo and head of cardiology [orig. overlege ved hjertemedisinsk avdeling] at Akershus University Hospital.
Ever since the start of the pandemic, doctors have been aware that the coronavirus can cause acute heart problems in seriously ill patients [seriously ill with Covid-19, as determined by a (drum roll) PCR test™, typically run in excess of 36-40 cycles (but I’m unsure: the two or so such tests™ I did in Norway never noticed the so-called cycle threshold); running such PCR tests™ (not a diagnostic tool) also shows, e.g., bird flu in dead polar bears and walrus, albeit only after 40-45 cycles, as we’ve learned to be ‘standard practice’:

Plus I’m old enough to remember this gem from 3 May 2020, which comes to us via (drum roll) Trusted News™ provider Reuters (source; archived):
Coronavirus test kits used in Tanzania were dismissed as faulty by President John Magufuli on Sunday, because he said they had returned positive results on samples taken from a goat and a pawpaw.
Magufuli … said the kits had ‘technical errors’.
The COVID-19 testing kits had been imported from abroad, Magufuli … instructed Tanzanian security forces to check the quality of the kits. They had randomly obtained several non-human samples, including from a pawpaw, a goat, and a sheep, but had assigned them human names and ages … Samples from the pawpaw and the goat tested positive.
I’ll spare us all the rest, but I’ll add this: do we know that the tests™ used in 2020 were the same as in, say, 2026? Oh, silly you and me, of course they are different, as per the CDC’s ‘Lab Alert: Changes to CDC RT-PCR for SARS-CoV-2 Testing’, issued on 21 July 2021, announcing changes to these protocols after 31 Dec. 2021. For the FDA’s two current (sic; also, whatever that means) guidelines, see ‘In Vitro Diagnostics EUAs - Molecular Diagnostic Tests for SARS-CoV-2’, issued on 24 March 2023 (and note that the original test™ could not identify any so-called ‘variants’ as it could only identify one target).
As regards cycle thresholds—which, once more, connects to the gold standard™ as per the polar bear and walrus story—back in 2020/21, let’s not forget that, e.g., Public Health Ontario instructed labs to run 38-40 cycles (17 Feb. 2021; source; archived) and their ‘splanation™ is hilarious1 and quite a tell; we note, in passing, that the FDA used a cycle threshold of ‘within 40.00 cycles’ as late as 7 March 2023 (archived), albeit with qualifiers, such as:
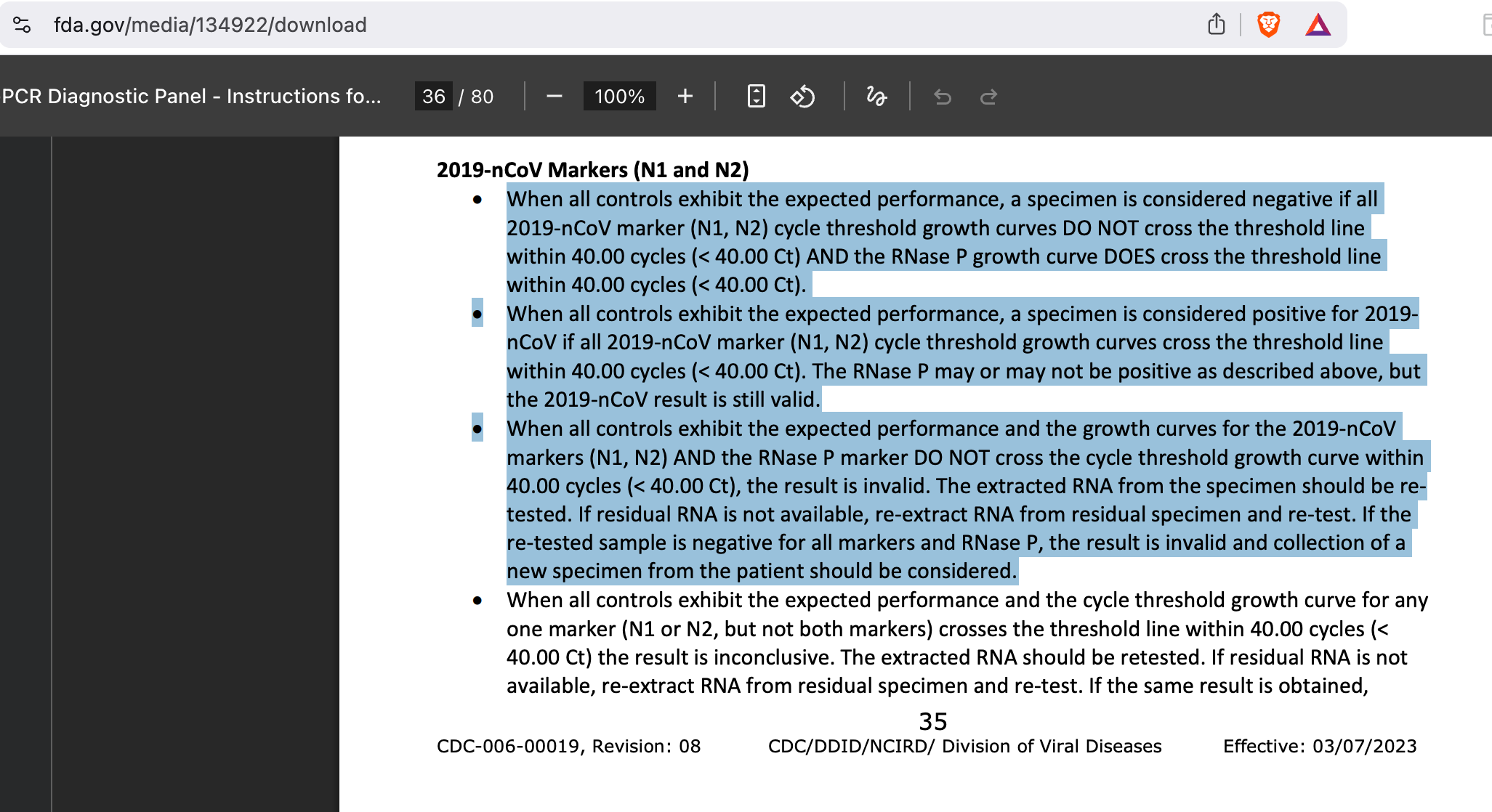
In case you’re asking, my personal favourite remains the third of these highlighted bullet points, which I’m reproducing here in a big quote:
When all controls exhibit the expected performance and the growth curves for the 2019-nCoV markers (N1, N2) AND the RNase P marker DO NOT cross the cycle threshold growth curve within 40.00 cycles (< 40.00 Ct), the result is invalid. The extracted RNA from the specimen should be retested. If residual RNA is not available, re-extract RNA from residual specimen and re-test. If the re-tested sample is negative for all markers and RNase P, the result is invalid and collection of a new specimen from the patient should be considered.
And with these facts in mind, let’s go back to Wilthil’s rah-portin™]
Now, a recent study based on data from the Trøndelag Health Survey (HUNT) shows that the virus also leaves invisible traces [orig. usynlige spor] in the general population [not to be outdone by shitty PCR testing™, I suppose, and in addition to ‘asymptomatic carriers’ of yesteryear, we’re now at ‘invisible traces’: is this the next frontier in virology and public health? As a follow-up, if I may: how does one identify, let alone determine and analyse, something that is ‘invisible’?]
The study, which was recently published in the renowned journal European Journal of Preventive Cardiology, has followed almost 20,000 healthy residents of Trøndelag over several years [all of these studies™ are, forever and ever, published in renowned™ outlets].
By comparing blood samples taken just before the pandemic with samples taken afterwards, the researchers have discovered a disturbing trend:
Those who have had a corona infection have a clear increase in the protein troponin in their blood.
[here follows a link to a recent piece, which we’ve discussed here:

It basically tells everybody that ‘off-label’ use of poison/death juices can be beneficial (for Big Pharma and their minions in public health); as to the study, I’ll discuss this below Wilthil’s rah-portin™]
Hidden Strain on the Heart
Troponin is a marker of cardiac stress. When heart cells are damaged or exposed to great strain, this protein leaks into the blood.
When the level of troponin rises, the risk of suffering from heart disease in the future increases. This primarily applies to heart failure, but also heart attacks and strokes.
Thus Omland, who led the study, who emphasises that this is a so-called subclinical injury.
This means that the increase [in troponin levels] is so low that the values usually stay within what the laboratories define as the normal range [this is how one PHEICs another problem—it’s the Hegelian dialectic at-work: declare what is within ‘the normal range’ a problem™, add Big Pharma products™ as solution™, and usher in a New Normal, as in: the normal range of troponin levels is now dangerous™, administer heart disease meds, and profit handsomely—rinse and repeat (here’s looking at you, cholesterol levels from the 1960s, because we’ve talked about cycle thresholds a moment ago)].
Those who are affected do not notice anything in their everyday life and feel completely healthy [but da Science™ knows, just knows, they are not healthy; also, shouldn’t we all just affirm these feelies?]
Nevertheless, these findings are not insignificant [a declarative statement by journo™ Wilthil, let’s not forget that]. At the population level, chronically elevated troponin levels over time are strongly linked to an increased risk of developing real heart disease later in life, according to Omland [surely the good professor knows that ‘at the population level’ is as meaningless an analytical category as, say, ‘asymptomatic disease burden’, right? Right.]
[here follows an info box; as source, the Store medisinske leksikon is given)]
Troponins are a group of proteins found, among other things, in muscle cells in the heart.
In the event of damage to muscle cells, such as a heart attack, troponins leak into the bloodstream, and the amount can be measured with a blood test.
Normally, the troponin values in the blood are very low, but in case of damage to the heart muscle cells, the troponin value can multiply.
Moderate increases in troponin can be seen in other acute heart diseases such as heart failure, inflammation of the heart muscle (myocarditis), and heart rhythm disorders. [end of info box]
[Omland] In general, an increase in troponin reflects a fairly significant increased risk of heart failure, even with changes within the normal range.
On average, troponin levels increased by 4 per cent in those examined who had undergone Covid-19. Some had much higher levels [fun factoid: this is what the paper by Omland et al. notes as regards infection vs. ‘immunization’ (i.e., taking the poison/death juices; also, there word, not mine):
With regard to immunization for SARS-CoV-2, the [sic] vaccine [as if that’s the same concoction used over time (it’s not)] elicits spike protein IgG and not nucleocapsid IgG, a serological profile separating immunization from infection. Accordingly, we did not use values of spike protein IgG to evaluate infection status, as these values would be disturbed by vaccination.
I’ve now cursorily looked at some of the diagnostic tools used to identify IgG, specifically ‘PlaIgGCovSpi@NT4CovM (Plasma Immunoglobulin G Covid-19 Spike)’ and ‘PlaIgGCovNuc@NT4CovM (Plasma Immunoglobulin G Covid-19 Nucleocapsid)’, both of which, in their respective sections on ‘limitations’ (on p. 5 and p. 4, respectively), hold that ‘Negative results do not rule out SARS-CoV-2 infection’ and that ‘the persistence of a SARS-CoV-2 immune response has not been fully established. Negative results may be observed due to a decline in antibody titer over time’. But at this point, whatever is the way to go].
The study shows that those who had been infected by the coronavirus were 17 per cent more likely to have an increase of 50 per cent or more in the heart damage marker troponin [fun factoid: ‘98.9% of participants reported that they had received SARS-CoV-2 immunization’, again, their words, not mine—note the absurd, Orwellian use of ‘immunisation’—and consider the fact that there’s virtually no control group (of so-called unvaccinated™ people in the sample™].
[Omland] We also see changes in younger people [who also, to the tune of some 98.9%, got the poison/death juices]. An increase in troponin after Covid-19 may reflect an increase in the risk of heart disease in the long term [tell me we’ve got a problem re these poison/death juices in a way that obfuscates reality as-is, in particular for morons and low-information NPCs, such as journo™ Wilthil].
The fact that the increase is measured several years after the infection itself suggests that the virus can contribute to damage to the heart muscle, which persists long after the acute illness [do re-read the above-reproduced ‘limitations’ of these test kits used to determine this (or not)].
This is described as a condition where the heart muscle is under chronic low-grade stress, without it causing physical symptoms [just yet].
IPH Urges Caution
The Institute of Public Health (IPH) is following the research closely, but stresses that the findings must be interpreted with caution [yeah, to me, mainly, if not exclusively, because of the 98.9% vaxx rate of the participants: change my mind].
Division director Hanne Gulseth believes the study is interesting [I’m sure it is], but that the evidentiary base is not currently sufficient to conclude that Covid-19 increases the risk of heart disease in the long term. Thus Gulseth:
The study does not show whether this is a change that persists or whether it is temporary. It is also uncertain what significance such subclinical troponin changes have for future cardiovascular disease in the individual.
According to Gulseth, there are several reasons why someone has higher troponin levels in the blood—everything from various heart diseases, blood poisoning, chronic kidney disease and hard physical exertion—to certain drugs and medicines and the way the sample is analysed [we’ll have a go at these issues below].
She points out that the changes in the amount of the cardiac stress marker are small, and that they are within the range described as subclinical:
[Gulseth] It is still uncertain how such small increases should be interpreted, and what significance it has for the individual’s actual risk of disease. It is therefore important to have more studies and a longer follow-up period to gain more knowledge [thus the grift continues].
‘It is likely that covid-19 is the cause’
However, Omland says that the researchers have adjusted for other factors, and that it is likely that Covid-19 is the cause [note the singular, as well as the little confounding factors relating to PCR testing™, the ‘limitations’ to the IgG assays used, and the 98.9% vaxx rate of the participates: I’m sure Covid-19 is a lot of things, but it ain’t ‘the cause’]:
There could theoretically be other factors that coincide with Covid infection, but the analyses take this into account and it is less likely.
Gulseth at the IPH believes that the findings must be seen in a wider context. She points out that other respiratory viruses can also affect our cardiovascular system [also, get a boosta™ for whatever to help with this, right? Right.]:
We know from before that the flu can also cause a similar increase [yeah, incidentally, where did the flu go in 2020/21?].
[Wilthil] Does this provide grounds for the IPH to change or update its assessments regarding late-onset injuries from Covid-19 or follow-up of heart health after the pandemic?
[Gulseth] The IPH assesses such results in the light of the overall research in the field. This study alone does not provide grounds for changing our assessments.
Recently, NRK reported that the use of cardiovascular drugs has increased sharply among young adults aged 18–44 after the pandemic [yeah, we talked ‘bout that, too:

Bafflement™ ensued while tumbleweed is blowing through the hallowed hallways of public health institutions (and journos’ minds)]
Gulseth believes [sic] that there is no basis for believing that this is related to the results of the study:
It is likely that several different explanations contribute and work together to increase the use of drugs against cardiovascular disease in young adults. There is currently no basis for linking this directly to this HUNT study, but the study contributes to the knowledge base for our work in the field going forward.
‘The long shadow of he pandemic’
Independent international experts, however, describe the findings as ‘the long shadow of he pandemic’, and that this confirms [sic; they’re using the same data] that the coronavirus [sic] has left a measurable, physical residual damage to the heart in a large part of the general population [this is too funny not to mention: these are no typos on my part, and, admittedly, the Norwegian wording used by journo™ Wilthil—‘Pandemiens lang skygge’—is orthographically and grammatically correct—but the header of the underlying paper (to which Mr. Wilthil links once again) is this (timestamp: Monday, 8 June 2026, 6:09 a.m. Oslo summer time):
I’m sure this will be changed (by which I mean: memory-holed) in due time …]
The experts who have assessed the study say that this proves that the increase [in troponin levels] is not just due to a minimal change in fluctuations for everyone, but that a significant group has actually had a real and marked jump in troponin levels, which thus signals heart damage [remember: 98.9% of study participants took poison/death juices].
According to Omland, there is no reason to suspect that it is the vaccine, and not the virus itself, that is behind it:
We consider it very unlikely [this will not age very well].
The researchers have measured specific antibodies in the blood, which allows them to clearly distinguish between the immune response from the vaccine and a real infection [fun factoid: re-read the above excerpts concerning the limitations of the used assays].
No Reason to Run to the GP
Although the study provides new insight into how the virus affects public health in the long term, Omland emphasises that there is no reason for unnecessary concern, or to go to the GP to demand to have your own troponin levels measured:
I think that is of little use, especially if you have not measured troponin before the pandemic [who did? Those with cardiovascular problems, who were likely to get juiced asap due to them being a vulnerable™ group, hence we get the functional equivalent of the so-called ‘healthy vaccinee bias’, only working the other way: most, if not all, who did troponin testing before 2020 did so because of (drum roll) cardiovascular issues: it’s the perfect self-fulfilling prophecy]. If you only have one value after the infection, it is difficult to interpret it [well, there’s one underlying variable that affects 98.9% of the sample, you know, jus’ sayin’ …]
Omland emphasises that most of those examined only had slightly higher levels of the cardiac stress marker.
But since so many have been infected with the coronavirus, he still believes that this will have an effect from a public health perspective:
[Omland] In some who may be vulnerable due to other risk factors, Covid-19 may contribute to an increased risk of developing symptoms of heart disease.
Omland et al. (2026), or: Orwell Gives his Regards
I think if you replace the term ‘Covid-19’ with ‘poison/death juice-induced carnage’, both the journo™ piece and the underlying paper work quite well.
While I also think I’ve covered ± all that needs to be said, here are, as promised, a few choice quotes from the paper ‘Impact of SARS-CoV-2 infection on subclinical myocardial injury in the general population: the Trøndelag Health Study’, European Journal of Preventive Cardiology (no linked references):
Study Overview
The Trøndelag Health Study (HUNT) is the largest population cohort in Norway, spanning four waves from 1984 to 2019; HUNT1 (1984–1986), HUNT2 (1995–1997), HUNT3 (2006–2008), and HUNT4 (2017–2019).16,17 All participants from HUNT4 were invited to participate in a follow-up visit (HUNT COVID) [so, the underlying comparator data is about something completely different] …
Participants
The current study includes data on 37 823 participants from HUNT4 (pre-pandemic) with measurement of cTnI. Of these, at HUNT COVID (post-pandemic), 19 552 participants had repeat measurements of cTnI, and 19 550 participants had measurements of SARS-CoV-2 spike IgG and nucleocapsid IgG (Figure 1) [remember that neither test is a) consistent from 1984 through 2019 (or beyond) and that b) significant limitations as regards the reliability are mentioned (and cited above) in the supplementary documentation, but never-mind, esp. as the cycle threshold BS is also there for your consideration] …
Diagnostic testing for SARS-CoV-2
In Norway, diagnostic testing for SARS-CoV-2 evolved [sic] from 2020 through 2023. Initially, during the pandemic, the limited testing capacity was prioritized for symptomatic people, healthcare workers, elderly care, suspected outbreaks, and for hospital admissions. Intensive contact tracing, together with testing, was central to the national containment strategy. PCR testing was the primary diagnostic tool, with rapid antigen tests introduced in late 2020 as a supplement. During 2021, the testing volumes were expanded, with PCR testing more available to the general public. As immunization became available, targeted testing for high-risk groups became more common during 2022. Towards the end of 2023, testing became more selective and surveillance-based, and many free testing services were reduced or ended.
Setting aside all the nonsense about who went to get tested™ as often and as long this was offered for free™ (i.e., taxpayer-funded), which also affected test-positivity rates etc. and hence the prevalence of Covid, please consider when most study participants actually tested positive™ (it’s in the appendix):
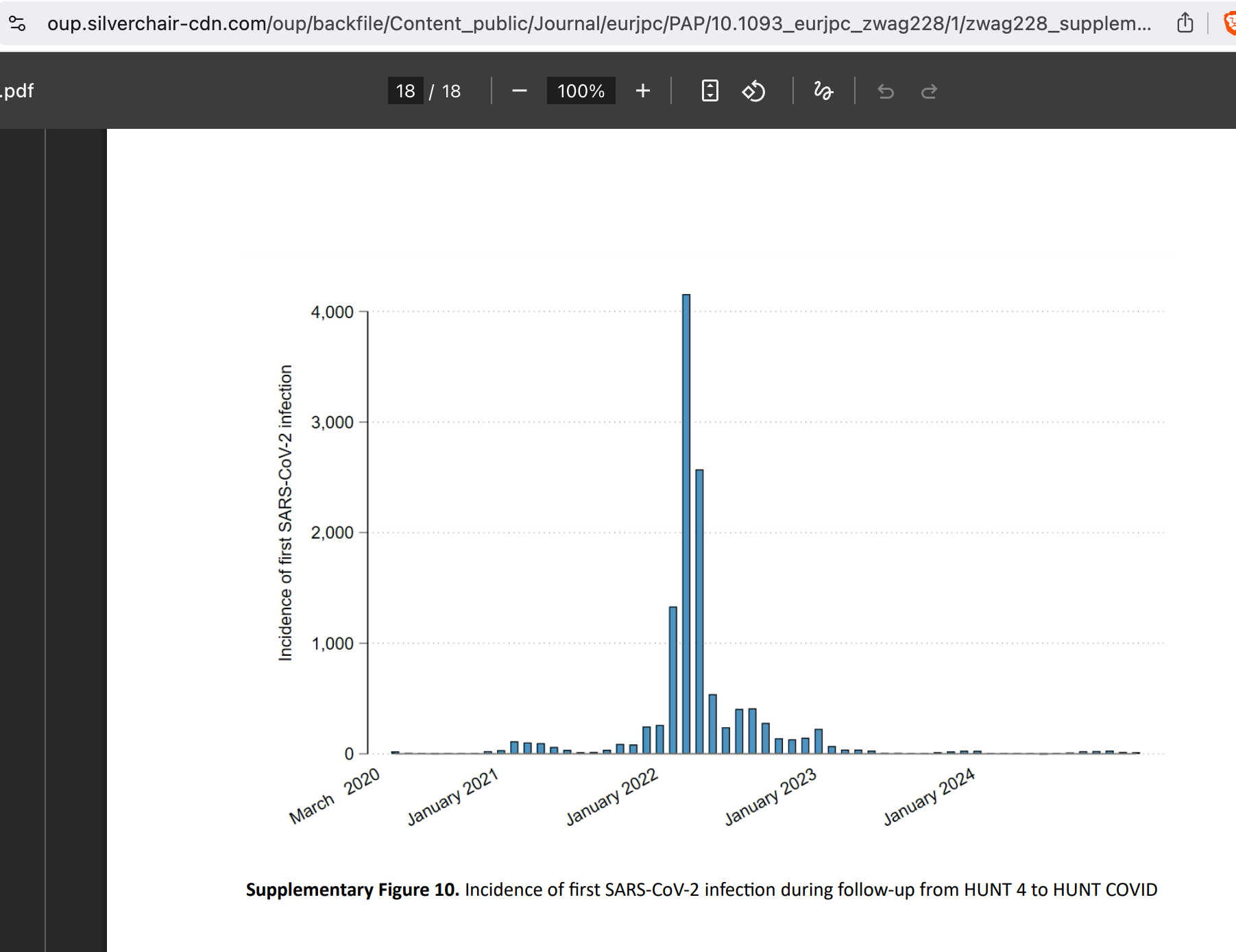
Oh, look, in-between the time elapsed, both availability, the test kits, and the guidelines as to who and how many times one would get tested™ changed (plus the CT tresholds). In case you’re wondering how this affected the data, well, I do wonder, too, but that thought isn’t troubling our intrepid experts™.
Outcomes
All participants provided data on their history of SARS-CoV-2 infection. The self-reported data from HUNT COVID [oh, look, the least reliable form of data, what a surprise™] was supplemented with data from the Norwegian Surveillance System for Communicable Diseases (MSIS), as all SARS-CoV-2 positive polymerase chain reaction (PCR) tests are reported to MSIS. Data on cause-specific mortality were obtained from the Norwegian Cause of Death Registry. All data from registries was obtained through 31 December 2024 [note that vaccination uptake data isn’t mentioned] …
We used a composite SARS-CoV-2 infection outcome (first event of self-reported or laboratory-verified SARS-CoV-2 infection or SARS-CoV-2-related death (ICD-10 codes U07.1 and U07.2)), as well as for the individual parts of the composite outcome separately. Due to the low number of SARS-CoV-2-related deaths, these models were parsimoniously adjusted for age, sex, eGFR, and history of cardiovascular disease [but not for poison/death juice update] …
Outcomes
Immunological indices of SARS-CoV-2 infection and subclinical myocardial injury
At HUNT COVID, 98.9% of participants reported that they had received SARS-CoV-2 immunization. Both SARS-CoV-2 spike and nucleocapsid IgG were linearly associated with post-pandemic concentrations of cTnI (Supplementary material online, Figure S2 and Supplementary material online, Figure S3). We used concentrations of SARS-CoV-2 nucleocapsid IgG as a proxy for immunological SARS-CoV-2 infection, with values <0.2 denoting SARS-CoV-2 naive persons, values 0.2 to <1.4 denoting previous infection, and values ≥1.4 denoting recent infection. Mean pre-pandemic cTnI was similar between all three groups, and the mean post-pandemic cTnI was higher both in persons with previous infection (1.96, 95% CI 1.91–2.00 ng/L) and in persons with recent infection (2.01, 95% CI 1.96–2.06 ng/L). Persons with previous or recent SARS-CoV-2 infection had proportionally higher post-pandemic concentrations of cTnI. Persons with recent SARS-CoV-2 infection were at a higher risk of increasing concentrations of cTnI and at a lower risk of decreasing concentrations of cTnI (Table 2; Supplementary material online, Figure S4 to S6).
Remember, 98.9% of participants took any number of poison/death juices.
Clinical SARS-CoV-2 infection and chronic subclinical myocardial injury
Mean pre-pandemic cTnI was higher in persons with no self-reported or laboratory-verified SARS-CoV-2 infection [that would be those who ‘only’ took any number of poison/death juice injections], and mean post-pandemic cTnI was higher in persons with self-reported or laboratory-verified SARS-CoV-2 infection (1.99, 95% CI 1.95–2.03 ng/L) [remember that both PCR and antigen/lateral flow tests™ don’t look for stuff from the poison/death juices, i.e., setting aside the ‘self-reported or laboratory-verified SARS-CoV-2 infection’ ruse, we’re still talking about a sample that’s 98.9% vaxxed]. Persons with self-reported or laboratory-verified SARS-CoV-2 infection had proportionally higher post-pandemic concentrations of cTnI [of the sample that’s 98.9% vaxxed]. They had a higher risk of increasing concentrations of cTnI and a lower risk of decreasing concentrations of cTnI (Table 3; Supplementary material online, Figure S7 to S9).
I’ll interrupt the flow to present you with that Figure S9:
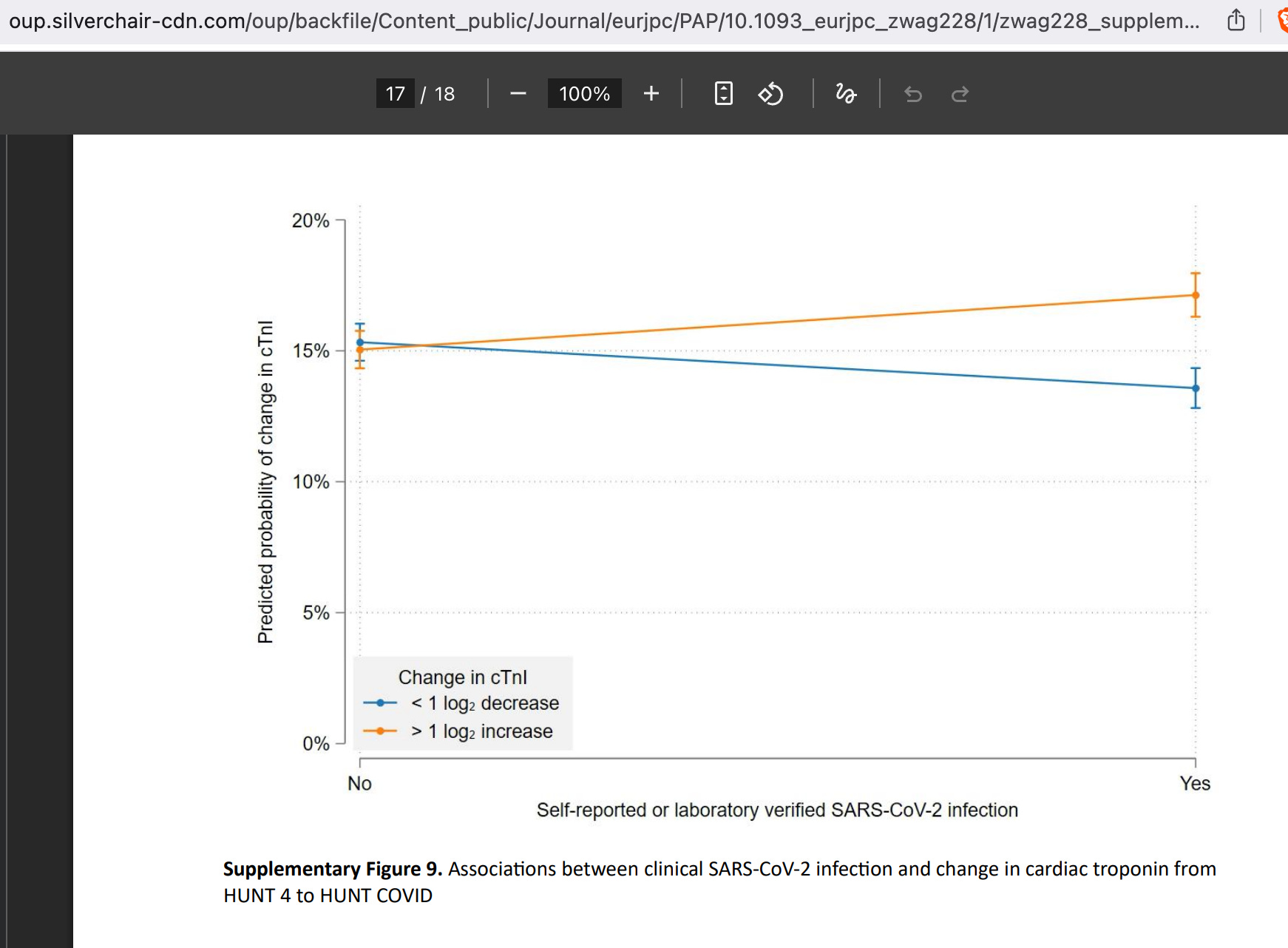
Note that if there was no effect (among the 98.9% vaxxed study population) and the ± poison/death juice intake, these lines would point in the same direction.
The results were comparable when analysing self-reported SARS-CoV-2 separately (Supplementary material online, Table S2). There were no associations between laboratory-verified SARS-CoV-2 infection and cTnI (Supplementary material online, Table S3).
Remember: Covid tests, be they of the PCR or antigen/lateral flow garden variety, are primed (designed) to determine infection, not poison/death juice stuff; i.e., that’s perfectly in line with infection vs. poison/death juice uptake differences. Or, in the FDA’s very own words as of 29 Aug. 2024 (source; archived):
Antibody (or serology) tests are used to test for the presence of antibodies from previous infection or vaccination and can aid in fulfilling the case definition for multisystem inflammatory syndrome in children (MIS-C) and adults (MIS-A).1 Antibody testing does not diagnose current infection. Antibody testing is primarily used for public health surveillance and epidemiologic purposes. Antibody tests detect specific antibodies that target different parts (nucleocapsid or spike protein) of the virus. Detection of anti-nucleocapsid antibody indicates SARS-CoV-2 infection, while anti-spike protein antibody may be induced by COVID-19 vaccination or by SARS-CoV-2 infection.
From the paper’s discussion:
These findings do not suggest a transition to overt myocardial injury at the individual level but rather a subtle shift in chronic low-grade myocardial injury at the population level and should primarily inform pathophysiological understanding of the long-term cardiovascular implications of SARS-CoV-2 infection.19
Remember, we’re talking about a 98.9% vaxxed study population.
Results indicate that high cardiac troponin is not associated with a higher risk of contracting SARS-CoV-2 infection.
There goes the reflexive inclusion of cardiovascular issues into ‘vulnerable groups’.
The above sentence is directly followed by this declarative statement of expert™ bafflement:
This paradoxical [sic; their word, not mine] finding is most likely explained by different risks of exposure, testing patterns, and health behaviours, rather than a protective biological effect of cardiac troponin. Individuals with higher cardiovascular risk profiles and higher cardiac troponin may have been more intensively monitored, more inclined to limit social contacts, and more likely to adhere to protective measures and testing recommendations.
This is as close as Omland et al. get to pointing to the ‘protective measures’ including, you know (and drum roll) the poison/death juices.
Translated from the academese, we learn that those who were placed in ‘vulnerable groups’ were told consistently that they were at high-risk for whatever (though that’s now quite seriously called into question in light of this paper) and hectored to get all juiced up.
Hence I’ll cite the below snippet from journo™ Wilthil’s discussion™ for the sake of record-keeping:
According to Omland, there is no reason to suspect that it is the vaccine, and not the virus itself, that is behind it:
‘We consider it very unlikely’ [this will not age very well].
Returning to this point, here’s what Omland et al. noted re: poison/death juices in their discussion (and we’ll also wrap this up now):
Pertinent to this notion, COVID-19 immunization is more frequently associated with direct myocardial injury and less symptoms [i.e., you get heart inflammation out of a blue sky, so to speak from the poison/death juices], while the inflammatory syndromes and cytokine storm in fulminant SARS-CoV-2 infection is to a larger degree correlated with the clinical course of the infection.28 [remember also that the first 14 days post-injection you’re counted as ‘unvaccinated’] As such, widespread immunization for SARS-CoV-2 might have influenced cardiac troponin concentrations by mechanisms other than those caused by the infection on its own.
More equivocation, but I read this as ‘maybe yes/no’, followed by a ‘we cannot say this due to the implications of having virtually everybody vaxxed and they might get angry’, to say nothing about, you know, liability issues.
Last quote from the paper (pinky-pie promise):
We demonstrate with higher confidence the detrimental impact of SARS-CoV-2 infection on cardiac health in COVID-19 survivors.
I call BS because the sample is 98.8% vaxxed, given the distribution of infections (see above), this occurred primarily during the Omicron™ wave in late 2021 and early 2022 when the boosters™ were widely taken in, hence we’re talking virtually complete vaccine failure (or poison/death juice failures doing what they were supposed to be doing) and hence that virtually all these infections™ are so-called ‘breakthrough infections’.
In other words: is it really logically defensible to make such statements while ruling out the poison/death juices?
Bottom Lines
Another day, more BS, gaslighting, and obfuscation from both experts™ and journos™ alike. Yeah, it’s easy to pile on journo™ Wilthil, but the paper, too, is quite a bit of an exercise in disingenuous double-talk.
Plus the comments offered by professor Omland are … well, despicable.
But, hey, it’s all the fault of Covid-19, right? Right.
Never-mind the fact that 98.8% of the study population took any number of poison/death juices and that the IgG assays cannot rule out infection or ‘immunisation’ (their words) as regards the proximal origin of elevated troponin levels.
Setting aside these next-to-irrelevant issues, the paper is da Science™ at its best, to say nothing about the extra-shitty bullcrap masquerading as rah-portin™ by journo™ Wilthil.
Lala-Landia continues.
And I shall quote:
At PHO, we have developed a PCR test in our lab, with positive and negative cutoff points. The cutoff point for a positive result for PHO’s developed lab test is 38 cycles. This means that if the virus is found at or before 38 cycles are completed, then the test is considered positive. The cutoff point for a negative result is 40 cycles. If the virus is detected between 38 and 40 cycles, we call this an indeterminate or inconclusive result. All inconclusive results are considered probable (likely) cases for public health reporting.
What are cycle threshold values?
The cycle threshold (Ct) value is the actual number of cycles it takes for the PCR test to detect the virus. It indicates an estimate [their word, not mine] of how much virus was likely in the sample to start with—not the actual amount. If the virus is found in a low number of cycles (Ct value under 30), it means that the virus was easier to find in sample and that the sample started out with a large amount of the virus. Think about it like the zoom button on your computer, if you only have to zoom in a little (zoom at 110%), it means that item was big to start with. If you have to zoom a lot (zoom at 180%), it means that the item was small to start with …
Why aren’t cycle threshold reported on test results?
Like with other PCR tests (including non-COVID-19 tests), it is not recommended to provide Ct values on test results in Ontario (and Canada). PCR tests tell us if the virus is present or not in the sample provided to the lab; however, there are other factors to consider in interpreting lab results [once again, their words, not mine]. Ct values are not directly comparable from one PCR test kit to the next, and can change with increased transportation times, sample storage conditions, and sample collection method [so, every PCR test result is … unique? How does that provide a shared baseline?].
Because of this, Ct values can help support lab specialists in validating results as well as reviewing complex cases. However, they need to be considered alongside the other important factors we discussed earlier—like exposure history and individual characteristics. At PHO, Ct values are available to health care professionals upon request, and low level detected results (Ct value 35 to 38) are indicated on the laboratory report (since November 2020). We also have specialists who are available to health care professionals who have any questions on interpreting lab results or want to discuss complex cases. There is still a lot to learn about Ct values and more research is required to fully understand Ct values and their link to disease onset, severity and infectiousness.
Since COVID vaccines are so effective, perhaps they can show the difference between those who had taken the jab and those who had not. Those who took the jab would naturally have lower rates of heart disease. ;-)
"Corona Infection"
What is that supposed to be?
THERE IS NO VIRUS!!!