
Norway, Sweden Report 'Sharp Increase' in Cardiovascular Drug Use Since 2020/21
‘This is a development that gives cause for real concern.' ∽ Magne Wang Fredriksen, secretary general of the Norwegian Heart and Lung Disease Association

Some time ago, it dawned upon Norway’s public health officialdom that something was off, that is, a feature of society’s post-Covid condition wasn’t quite right:


Of course, I could go on posting about this issue, but let me bring up one particularly shady character in all of this (and, no, I’m for once not talking about public health officials or the like)—NRK’s own journo™ Jan-Erik Wilthil. It is typically him who reports™ on the Covid shitshow, and if you would copy-paste his name into the search field of these pages, well, you’ll see.
His last contribution we discussed here was this:

But the other day, another of his pieces briefly appeared on the front page of Norwegian state broadcaster NRK (Friday morning local time), and it was quite literally gone within 1-2 hours; not ‘gone’ as in deleted, but ‘vanished’ from the main page.
Hence, hi Steve Kirsch, Dr Mike Yeadon, Sasha Latypova, el gato malo, and others, perhaps you’d wish to weigh in on this.
So, we’ll talk about it now, just to make sure that we’ll keep some of these receipts. As always, translation, emphases, and [snark] mine.

Sharp Increase: More Young Adults are Using Cardiovascular Medications
The use of medications for cardiovascular disease has skyrocketed among people as young as 18 in both Norway and Sweden. Researchers link the development to the coronavirus.
By Jan-Erik Wilthil, NRK, 15 May 2026 [source; archived]
‘My hands were shaking, I was sweating, and my heart was pounding. I also had problems with my vision’, says Sohaib Jubran Sheikh.
Three years ago, he learned that his blood pressure was dangerously high:
Blood pressure was measured at 240 in the hospital.
This is considered a critically high level that requires emergency treatment.
The alarm on the machine went off four or five times, and the nurse couldn’t turn it off. She called a doctor immediately.
The doctor insisted [sic; really?] on checking his blood pressure before they could let him leave the hospital.
Alarming Increase Among Young Adults
Now the 42-year-old from Oslo is part of a growing statistic of young adults using medications for cardiovascular disease.
Figures from the Norwegian Institute of Public Health show a sharp increase in use among people aged 18 to 44.
The use of these drugs has been increasing slightly for many years, but accelerated when the pandemic hit. The trend has shown no signs of slowing down.
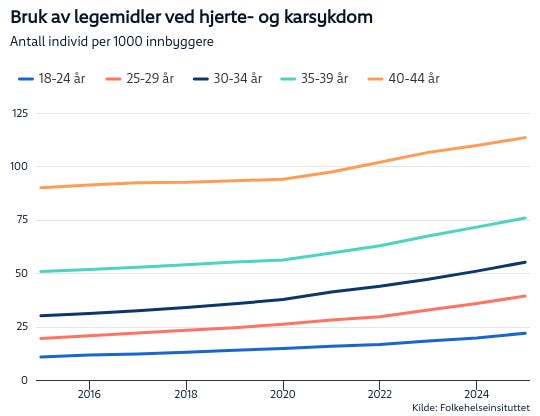
[This is the graph embedded into the piece, and even in this form of representation, the data speaks loudly—‘something’ changed in 2020/2021, and NRK journo™ Wilthil is to be commended for adding the underlying data™ in an Excel spreadsheet, which looks like this:
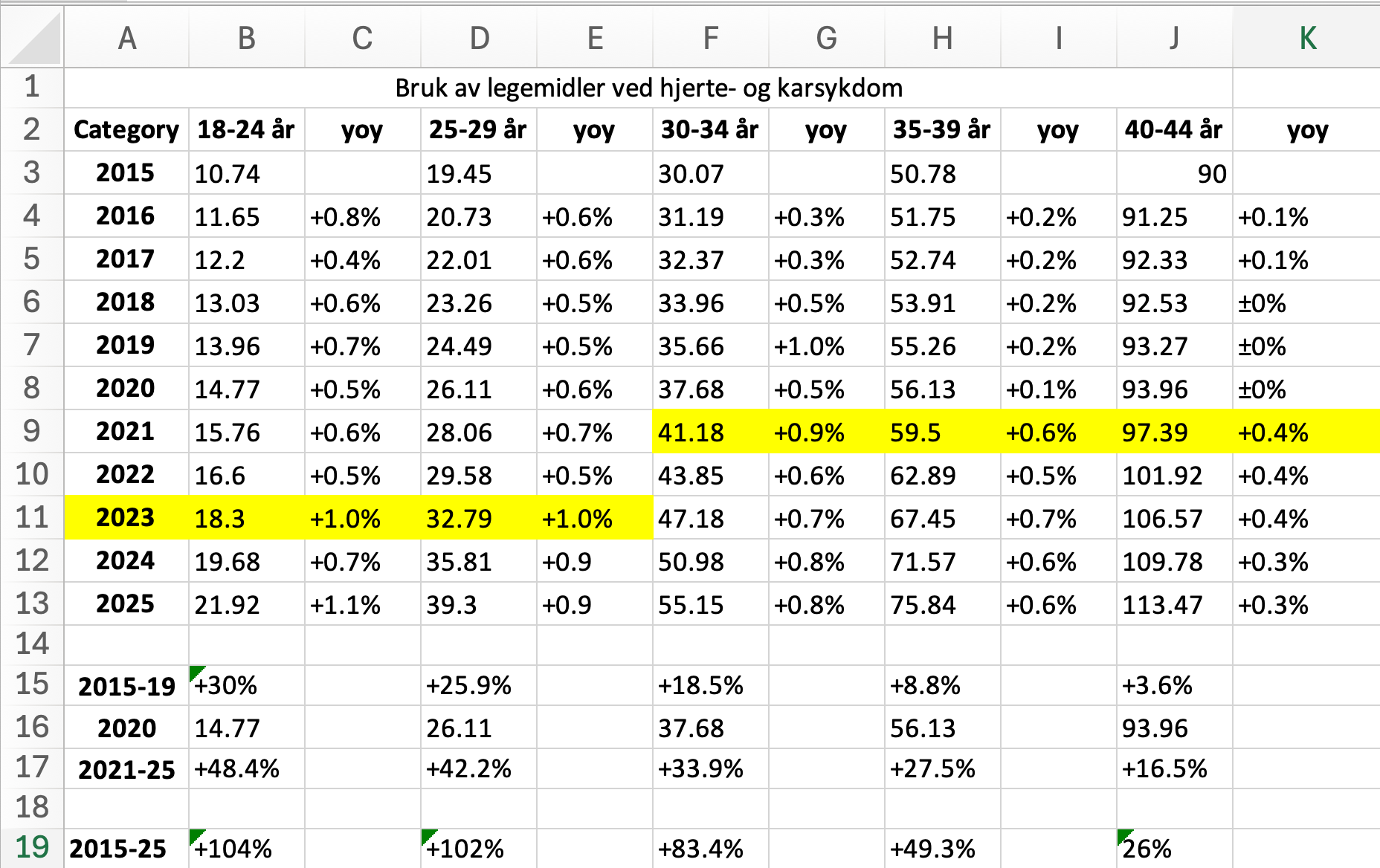
Note that I’ve added columns labelled ‘yoy’ (year-on-year changes) for each of the age brackets as well as the (sub)total changes in lines 15-17 and 19, respectively; the highlighted (in yellow) cells indicate the approximate timing of when sudden and unexpected increases in the incidence occurred, i.e., in 2023 for the age brackets 18-24yo and 25-29yo, as well as in 2021 for the age brackets 30-34yo, 35-39yo, and 40-44yo.
Now, all I’m saying is that in 2021/2023, there were quite big changes going on—the incidence doubled for young adults in their 20s as well as all but did so for the age bracket of 30-34yo whereas the incidence sextupled for 35-39yo and quadrupled for people aged 40-44yo.
All I’m asking you is to keep these numbers and the yoy changes in mind as you read on, for you’ll see that these changes are interpreted … well, see for yourselves]
‘Reason for Concern’
Last year, 37,700 more people aged 18 to 44 used medicines for cardiovascular disease, compared to 2019.
In the 18–24 age group, there is an increase of 57 per cent over the past five years [2020-25, a quite easily discernible accounting trick used by public health officialdom, which permits ‘masking’ of any effects that may or may not have occurred after 28 Dec. 2020].
Among those aged 30–34, the use of these medicines has increased by over 63 per cent in the same period.
‘This is a development that gives cause for real concern’, says Magne Wang Fredriksen, secretary general of the Norwegian Heart and Lung Disease Association.
He believes it is now urgent to find out what the cause is:
When so many more people, including young people, need this type of medicine, it is a signal we cannot ignore. It is now urgent to gain more knowledge about the causes, so that we can take the right measures, both to prevent disease and to ensure that medicines are used correctly.
[so, at least we’ve got the Science™ on the record noting that there is, in fact, a signal in these data; now, while I’m not a medical doctor, my first reaction is to ask the question—could it be that new drugs that were approved in the past decade are a potential, or possible, culprit here? But this is what comes next:]
The Secretary General believes there is reason to investigate whether the coronavirus could be an explanation [ahem, WTF? I mean, I’m quite sure, personally speaking, that the strange™, even perhaps baffling™, onset of massive changes—the doubling of the incidence for people in their 20s and worse increases for people in the 30s and 40s—in 2021 and 2023, respectively, is due to the poison/death juices, and I can ‘splain the chronological discrepancy, too: young people took but two injections early, with middle-aged adults topping off their ‘full vaccination course’ with one or more ‘boosters’, as, e.g., speedo-wearing public health expert™ Jörn Klein recommended to ‘young people’ as recently as autumn 2024].
[Magne Wang Fredriksen] When we see such a clear increase among younger people, it is natural [sic] to question whether Covid-19 may have contributed. There is international research that points to an increased risk of cardiovascular disease after infection, but we still lack clear answers. This is something we now need to gain better knowledge about.
IPH: ‘There may be several explanations’
The Norwegian Institute of Public Health (IPH) confirms the increase [well, it’s their bloody data, but whatever], but they are reluctant to conclude about the causes.
The increase in the use of cardiovascular drugs may have many explanations. We cannot ignore that having had Covid-19 infection may have had an impact, but we do not know this. We are concerned with producing and communicating reliable knowledge, not speculating, and being clear about what we know and do not know.
Thus Director Hanne Gulseth at the IPH [after a moment of clarity, the public health official then rambles on and (drum roll) speculates wildly].
She emphasises that increased use of these drugs may also be due to increased use of drugs in general, a greater focus on prevention, and changes in lifestyle and health service use both during and after the pandemic [it’s all and (almost) nothing in terms of possible causes, yet the poison/death juices must never-ever be mentioned as even a slight possibility, however small it may be].
[NRK’s Wilthil] To what extent is the IPH aware of this development, and what is being done to investigate this further?
[Hanne Gulseth] We at the IPH are monitoring developments in both drug use, morbidity, and mortality related to cardiovascular disease. These drugs help prevent serious illness and premature death. At the same time, it is important to follow developments closely and further investigate what is behind changes in use, especially among younger age groups [saying nothing while using as many expert-ey words as possible].
According to the IPH, there is a particular increase in the use of so-called beta-blockers, certain blood pressure-lowering drugs, and cholesterol-lowering drugs among those under 45 [yeah, we’ve seen these data].
Some of these drugs are used to treat other disorders such as anxiety, ADHD and migraine, but several of these drugs are omitted from the figures [so, the situation may actually be way worse due to accounting differences: good to know].
Few Cases of Myocarditis After Vaccination
‘It is important to note that the increase in the use of various drugs varies between gender and year. The use of beta-blockers is increasing more among women than men, and the increase started from 2015/2016’, says Gulseth.
According to director Gulseth, there has been a general increase in the use of several drugs among both children, adolescents, and young adults:
Increased drug use is positive when it helps prevent and treat existing diseases and ailments, but can also be a sign of more disease in the population or medical overtreatment.
At the start of the pandemic, it became clear that the corona vaccine could cause myocarditis in some people.
[I’m adding this one piece here—about a 20yo recruit who ‘almost died’ after taking the poison/death juice and received around US$ 200 in vaccine injury compensation:

And then we shall also note that the line ‘maybe Covid-19 did it’ has been peddled, falsely, I shall opine, since 2023/24, as this piece clearly shows:

Yet all we get from public health officialdom is this kind of inane ass-covering]
Gulseth believes that the number who experienced this side effect is too low for this to have contributed to the increase:
We estimate that less than 100 people under the age of 30 were hospitalised for myocarditis after corona vaccination. A separate clinical study led by Oslo University Hospital is following up this patient group to learn more about any lasting problems.
[that may factually be correct (see below), but let’s just quickly forget about 100+ seniors who died within the first couple of weeks of the roll-out of the poison/death juices on 28 Dec. 2020, which was assessed by the Science™ as ‘sad, but these were old geezers anyways’:

Plus there was a count going on among public health officialdom, specifically at the Medicines Agency (then Legemiddelverket, now Direktoratet for medisinske produkter, or DMP), whihc operates a dedicated ‘inflammation of the heart’ website, which shows this graph:
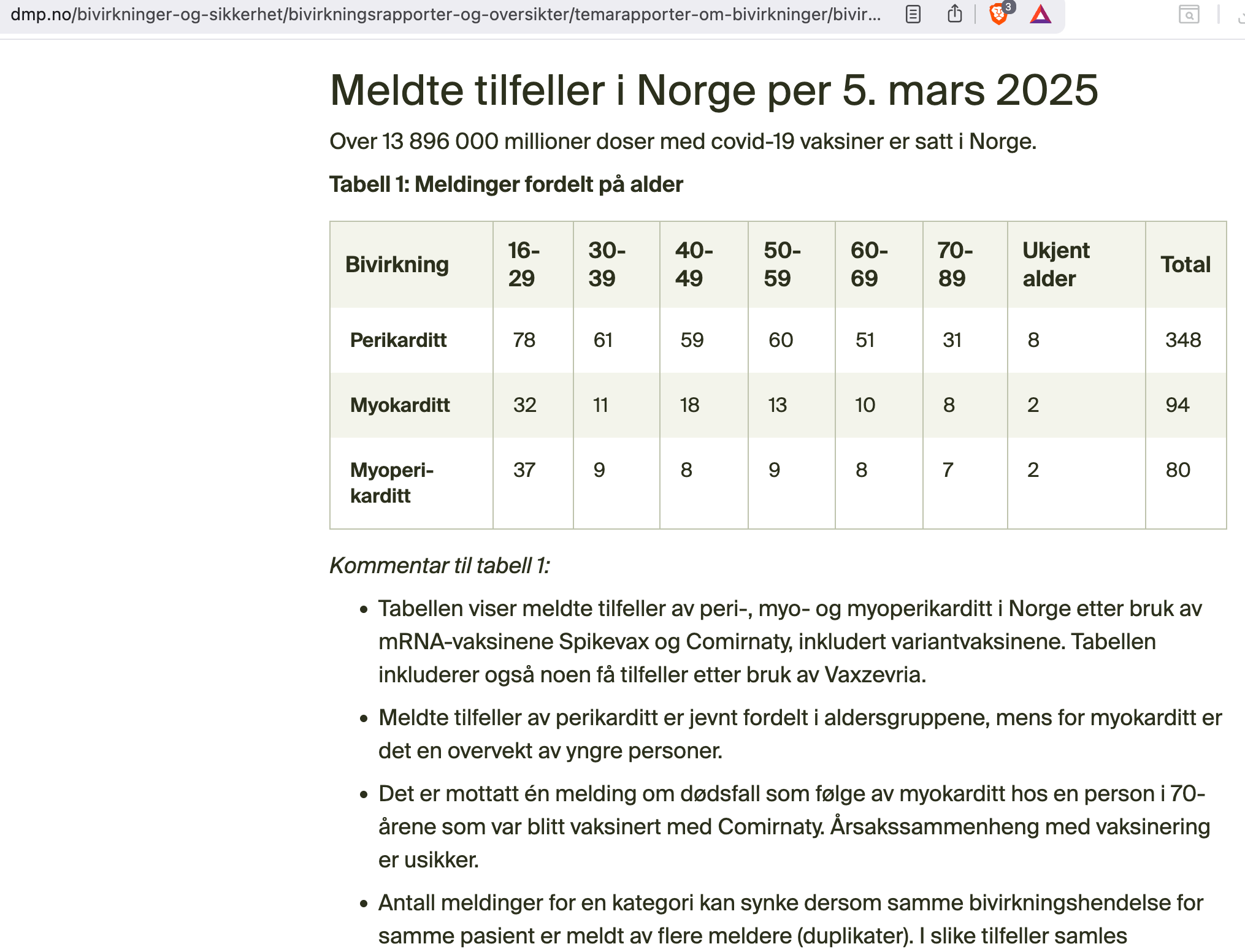
The above table is highly relevant (but note it’s technically impossible to compare to the above data used by journo™ Wilthil as the DMP inexplicably uses different age brackets) as it shows the total number of poison/death juice-induced myocarditis as ‘below 100’—and Wilthil lets IPH Director Gulseth get off lightly by not asking about pericarditis and/or myopericarditis: it’s gaslighting, or lying by omission, of the worst kind.
If you wish to follow-up by reading the DMP’s official ‘we’ve done the pharmacovigilance’ stuff™, please click here:

And now back to our intrepid journo™ Wilthil and his ongoing quest to gaslight the low-information people who read his crap]
Increase Also in Sweden
This development is not unique to Norway. In neighbouring Sweden, far more young people are also using the same drugs than just a few years ago.
Figures NRK has obtained from the Swedish Socialstyrelsen [National Board of Health and Welfare] show a marked increase among young adults. Here too, the development accelerated at the same time as the pandemic hit [note that here, too, journo™ Wilthil tells but won’t show you anything, hence my prompt expressed as a trendline—see if you can spot the inflection point…
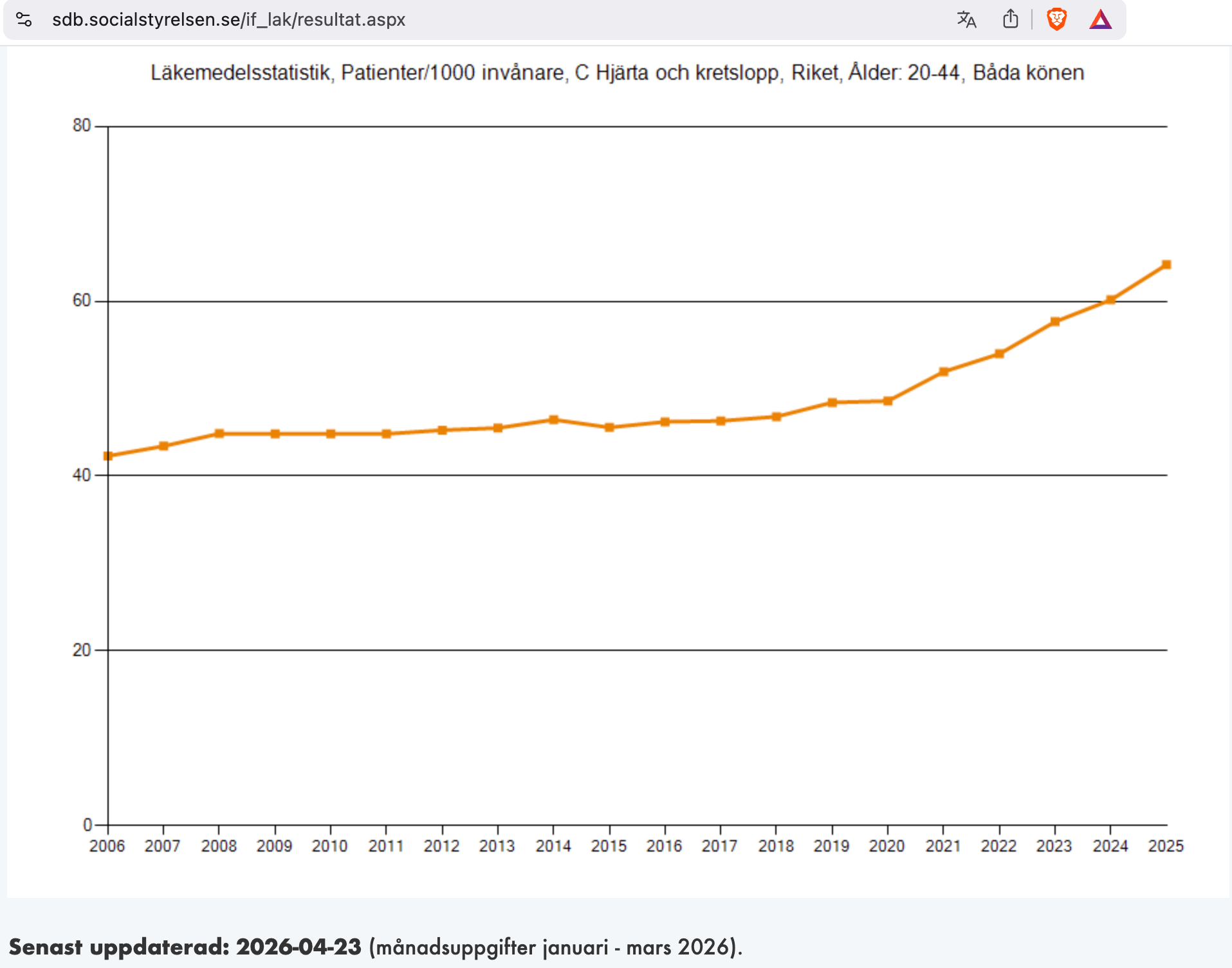
As per the underlying table (email me and I’ll send the Excel file), we get the following markers:
42.29/1,000 residents received cardiovascular drugs in 2006, by 2025, this figure had risen to 64.18/1,000 residents, a 51.7% increase
to compare these data with the Norwegian one related above, the Swedish baseline in 2015 was 45.55/1,000 residents, which increased to 48.41/1,000 in 2019, a 6% increase
in 2020, that number was 48.58/1,000 residents, and from 2021 (51.93/1,000) it increased to 64.18/1,000 residents in 2025, a 23.5% increase
over the entire ten-year period (2015-25), the increase in Sweden was 40.9%, with a marked change in the trend line in 2020/21
But nevermind reading journo™ Wilthil’s considerations, for you’d never be told that]
It is worrying that we are seeing such an upward curve [from 2020/21 onwards, mind you] in an age group [sic] that is otherwise rarely treated for cardiovascular diseases.
Thus cardiologist and professor Artur Fedorowski at Karolinska University.
He refers to a sixfold increase in Swedish prescriptions for the drug Ivabradine between 2020 and 2025 [the expert™ is baffled™].
According to Fedorowski, this may indicate that more people are struggling with heart rhythm disorders [yeah, it ‘may indicate’ this: are you TF kidding me?].
Swedish media have also reported a sharp increase in the use of so-called beta-blockers among young women aged 15 to 29 [haven’t read that one].
The professor believes this is possibly linked to the aftereffects of Covid-19 [of course the professor believes this; we note, in passing, what Kari Mullis once said: ‘Scientists don’t believe, they have evidence’, as cited by Celia Farber in her amazing Serious Adverse Events (Chelsea Green, 2023, p. 129)].
Fedorowski refers to a study published in the renowned medical journal The Lancet, in which he himself has participated [note two things: first, the magical incantation that the journal The Lancet is renowned, as if that means anything per se; second, setting aside the auto-referential nonsense, here’s the core sentence that tells you all you need to know about the study™:
The registry [used for the paper] does not capture certain lifestyle factors (e.g., physical inactivity, diet), vaccination status, or over-the-counter medication use—unmeasured confounders that may partially influence outcomes.6,8
So, the professor is technically correct in his belief; but since neither poison/death juice uptake nor over-the-counter drug intake is considered, that paper is also totally worthless in providing any answers to the baffling™ issue at-hand]
The study shows a clear connection between the diagnosis of Long Covid and an increased risk of cardiovascular diseases such as arrhythmias, heart failure, and blocked blood vessels, even [sic] among younger people [yeah, and I propose that this is because (drum roll) that study ‘does not capture… vaccination status, or over-the-counter medication use’, which is labelled ‘unmeasured confounders that may partially influence outcomes’: go figure].
‘It is an additional burden on society, both in the form of increased health costs and loss of working capacity in younger people of working age’, the professor points out.
Fedorowski has previously warned that the coronavirus can lead to high blood pressure [oh, really?].
Warned About Covid-19
Corona researcher and specialist in infectious medicine Arne Søraas has warned several times that Covid-19 can lead to later damage, also to the cardiovascular system:
There were early signals that Covid-19 caused cardiovascular diseases. That is why I have warned about the possibility of long-term effects, including heart disease, even after a mild course of Covid.
[if you can bear it, read this testament of insanity, courtesy of both journo™ Wilthil and the resident experts™ in Norway:

And take not of the date: August 2024]
He points out that the European Society of Cardiology concluded last year that the coronavirus can cause inflammation in the blood vessels, which in turn can lead to cardiovascular disease.
Søraas believes [more belief] that the Norwegian Institute of Public Health should now invite long-term COVID researchers and the Ministry of Health to a meeting to review the research in the area and look at what other countries are doing to reduce the infection:
Leading countries such as the USA have recommendations to stay home if you have respiratory symptoms, which will reduce infection [but won’t help you].
Last year, NRK met with the internationally renowned researcher David Putrino, when he was visiting Norway [he, too, is renowned].
At that time, the top researcher warned of more heart disease in the years ahead, as a result of repeated corona infections:
Covid-19 is a disease that also affects the cardiovascular system. If science is right, we will see an increase in these diseases in the future.
Suspects Covid-19
Sohaib Jubran Sheikh himself was hit hard by Covid-19 already in 2020:
I was on sick leave for at least twelve weeks. There were three months of continuous coughing. My lungs were really wheezing.
Since then he has struggled with various health problems [I have no way of knowing he took the poison/death juices, but my money is on, yes, he did]:
I have been in poor condition for two and a half years afterwards, and my stomach is still affected.
Now he suspects that the disease may also have triggered high blood pressure:
It fits with everything I have actually experienced and concluded. That it has caused enough damage to the body that it may have affected the heart and blood supply.
Bottom Lines
I’m merely keeping some of the receipts here, but you can clearly see how much gaslighting is in the reporting™ by journo™ Wilthil, as well as how much unwillingness to even consider the poison/death juices.
You know, the above piece also reminded me of some other reporting™, which is in line with these observations:
We saw, briefly summarised, how journos™ are publishing pieces that read like sieves, i.e., there’s so much that’s un-asked and un-mentioned, such as the stuff about when the trend in cardiovascular drug intake changed (2020/21).
It’s not ‘just’ in Norway—but also in neighbouring Sweden, which is roughly comparable in just about everything, hence we now have the recognition of corroborating trends.
We further notice the gaslighting of renowned experts™ in academia who deliberately exclude the poison/death juices (and other stuff) from their studies™ that later appear in, of course, renowned outlets, such as The Lancet.
One cannot find™ what one doesn’t look for, hence the above is both massively misleading and the equivalent of a drunk looking for his lost keys under a streetlamp, if only because there’s light at night.
Finally, I was also reminded of a longish exposé I did a while ago about the implausibly high incidence of (drum roll) cardiovascular problems affecting Norwegian top athletes:
There are eight such athletes with virtually the same cardiac issues while there are 1.85m people in the age bracket 20-44. Assuming 90% of these took at least 2 shots (c. 1,665,000 shots X two) plus about 50% of them a ‘booster’ (add c. 832,500 injections) = approx. 4.2m injections. If what Doctor Berger was accurate—1 in 100,000 injections came down with such cardiac problems, there should be no more than five or six such incidents.
You may wish to read up on this here:

Instead of following the first rule of holes (‘stop digging’), public health officialdom, journos™, and experts™ continue to lie to themselves—and to everybody else.
We’ve yet to reach rock-bottom. Brace for impact, because it won’t be pretty.
I'm hung up on the wrong thing, as per usual:
How can you call a 39-year old man a "young adult"? And is it a coincidence that they picked someone who is obviously not a Norwegian, to represent "young adults" in Norway?
About the data:
It is becoming increasingly common, I find, that people on the side of Authority tries to call any data-point they do not like for anecdotal, and to trot out the old "correlation is not causation" (demonstrating that they understand neither term) - well, data is a collection of correlated anecdotes, when you break it down.
Aggregated anecdotes is the kind of thing you can say that makes statisticians want to slap you.
Thank you.
From my recollection, Sweden allowed infection of the population before the majority was vaccinated. Once the infection had passed through the population, there was a drop in deaths as one would expect for a 'harvesting' effect of a seasonal infection that affects the frail and brings deaths forward by a season. Then people in Sweden suffered lower excess deaths than many other countries that vaccinated people before they were infected (eg New Zealand, and Australia in which people in WA and QLD were vaccinated comprehensively before infection). To me it looked as if infection could give protection not just against further infections but against the injections too. But I'm not sure what happened in Norway? I thought the virus was restricted in Norway to some extent, at least more than Sweden, so I would expect some differences between these two countries in excess deaths in the covid and vaccine years, and in cumulative excess deaths over following years (and related changes in life expectancy). Are you aware of differences in mortality, or in other symptoms such as high blood pressure, between Norway and Sweden?