


Covid in Norway: Crapification of Data Accelerates, but what's available shows it's a 'Pandemic' of the 'Boosted'
Compared to the 'unvaccinated', booster recipients are 10X as likely to end up in the hospital for Covid-19, 20X as likely to end up in the ICU, and 26X as likely to require ventilation

Prefatory remarks: for the past couple of weeks, I’ve struggled to find the right way (format) to assess the sudden changes to Norway’s sudden changes in how it reports on all matters Covid-19. True, the issue itself is almost gone from the public sphere, with all matters Ukraine-Russia having taken over discourse in the third week of March 2022. It’s a testament to the power of ‘the narrative’ to shift so suddenly, as if ‘led by an invisible hand to promote an end’ (to borrow from Adam Smith’s The Wealth of Nations, New York: Bantam, 2003, p. 364).
That said, this is a long post to account for these appropriately, so, perhaps you’d like to grab a cup of coffee or tea?
Q: what has changed that caused this (kind of) hiatus in my writing?
Well, it’s not that I’ve stopped writing about Covid in Norway in mid-March. I’ve documented the evolving adverse events (AE) reporting situation with two follow-up pieces on my larger three-part series on 15 and 17 March (see here and here). Both articles show that warning signs about these biological products were emerging literally the moment the first injections were administered.
Yet, nothing changed. No-one in charge—neither the Right’s (Høyre) politicians around then-PM Erna Solberg (who’s trying to regain power, by the way) nor anyone in the ‘public health authorities’ like Camilla Stoltenberg (Director of the Institute for Public Health, or IPH) or Preben Aavitsland (Head of the Infectious Diseases Division) are doing anything to stop the administration of these products.
While I personally don’t like to think myself as belonging to either one or the other side of the political spectrum (matters are too complex to filter them through a binary left-right matrix, I’m more interested in stances on issues, which vary over time and context), it’s important that the current left-of-centre coalition led by the Labour Party’s Jonas Gahr Støre places much less ‘emphasis’ on these issues.
To their credit, Mr. Støre’s government did a lot to reduce the power of the IPH by ending the latter’s participation in press briefings in January-February 2022, which preceded the abrogation of all mandates.
If you’d like to take a trip down memory lane, here are my bespoke pieces:
18 Jan.: a new data tool by the Health Directorate (Helsedirektoratet) allowed for the tracking of Covid-related and all-cause hospitalisations.
19 Jan.: looking at these data and the IPH’s weekly reports allowed for the comparison over time of rates of increase—turns out that ‘vaccinated’ individuals are far (more than a magnitude) more likely to be hospitalised than ‘unvaccinated’.
21 Jan.: when the IPH’s update for week 2 came out, no amount of (disingenuous) fudging of data—such as the introduction of the new and undefined category of ‘basic immunisation’ (2 injections)—could obscure the shifting trend lines: hospitalisations of triple-injected individuals were beginning to shoot up.
27 Jan.: by the end of that month, ‘vaccine failure’ had become too big to hide as the Omicron wave gained momentum: as we’ve seen in the two months ever since, these products don’t play much of a role, if any, when it comes to the current epidemic situation.
28 Jan.: this was actually recognised by the IPH, which revealed a number of important issues (but used different age brackets to do so), in particular age and population density to drive infections; finally, authorities suggested that kids better catch Covid-19 rather than get injected with these genetic ‘vaccines’.
The rest, as they say, is history: the government saw these reports and assessments—and concluded to do away with the mandates etc. I won’t detail my posts from February and March here (you can find them always by looking for the ‘Covid in Norway’ title), and instead I’d like to provide you with a concise update on the past couple of weeks now.
Big Change #1: no more ‘incidental’ infection-tracking as of week 10
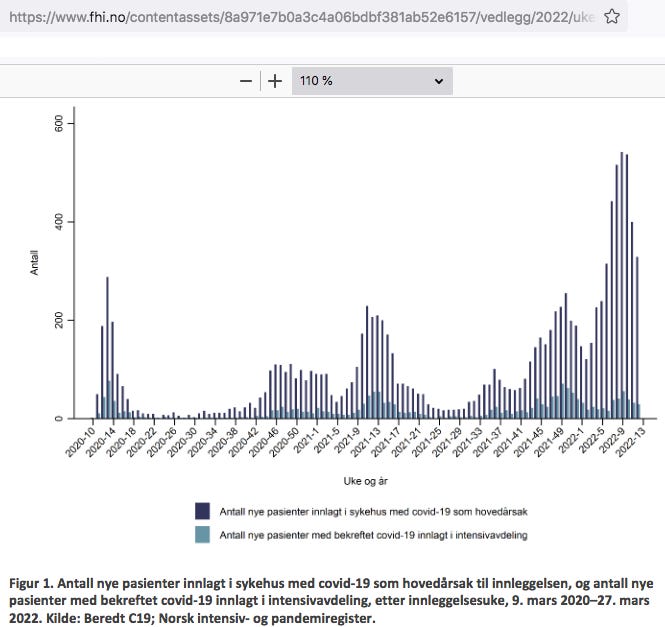
In my last report on the IPH’s update (week 9, see here), I suggested that the authorities’ own data on ‘incidental’ infections was revealing: these reports had long contained a figure that differentiated between hospitalisations for Covid-19 as main cause vs. ‘with’ Covid-19. In week 9 (Fig. 1), this graph looked like this:

On 10 March, I wrote that the ‘drastic rise in non-Covid admission since autumn 2021 reeks of potential immune suppression’. While I thought of this as a hypothesis, guess my dismay as none of the by now three further weekly updates included this figure.
From week 10 onwards, the graph looked like this (note that the below graph is from the current report, i.e., week 12, p. 8; for the two earlier reports, see the updates for week 10, p. 8, and week 11, p. 8, respectively):
Needless to say, without incidental Covid-19, it’s really hard, if not outright impossible to use these updates for anything other than, say, bean-counting.
Big change #2: no more public data due to a change of governmental policy
In my endeavour to somehow find these data, I ventured over to the Health Directorate’s daily updates—only to learn that they stopped providing these numbers:
From 23 March 2022, this reporting will be terminated and no more updates will be provided beyond this date.
As the bespoke press release held,
the Health and Welfare Ministry has determined that the daily reporting…of the number of Covid-19 hospitalisations, including six other variables, ceases.
In my world, the end of the IPH providing the data on ‘incidental’ Covid-19 coincided with the Health and Welfare Ministry’s decision not to share these same data, which, in turn, reminds me of Ian Fleming’s Goldfinger: ‘once is happenstance, twice coincidence, thrice is enemy in action’.
Why might these changes have occurred?
In practice, this means that any hospitalisations numbers provided by the Health Directorate will no longer (from 23 March 2022 onwards) show anything related to ‘Covid-19’:

The last bespoke data point notes 467 Covid-19-related admissions as of 22 March 2022.
Thus, the last complete week of data we may use to cobble together anything resembling a relational number would be week 11 (14-20 March), which holds that there were 373 new hospitalisations with Covid-19 as main cause of admission.
In the same period (14-18 March, for there is no data on these for 19 and 20 March in the data set I downloaded from the Health Directorate’s website), there were 2,744 admissions who tested positive for Sars-Cov-2.

In other words: for every admission with Covid-19 as main cause, there’s 13 admissions with ‘incidental’ Covid-19.
Is it too much to ask the Norwegian authorities whether or not this is the reason for the discontinuation of the publication of these data?
What’s the overall state of play w/respect to Covid-19?
Here’s the breakdown of the main points from week 12 (21-27 March 2022), all based on the IPH’s update (emphases mine):
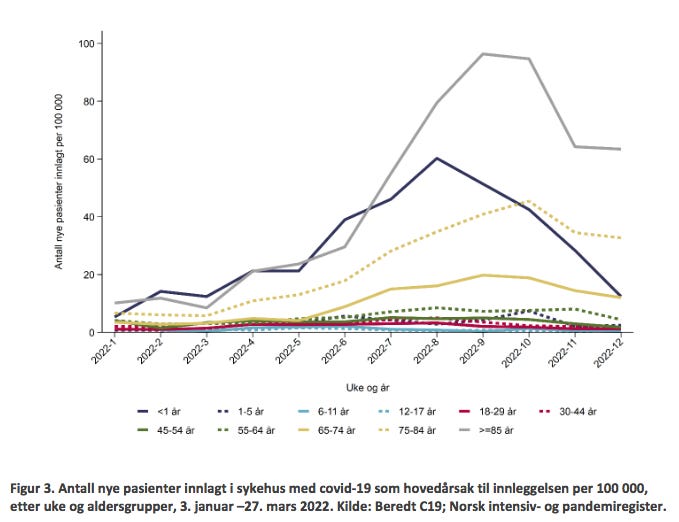
329 new admissions for Covid-19 as main cause, with the highest incidences per 100,000 among seniors (75-84 and 85+ yo); it appears that the Omicron wave as passed now.
As regards Covid-associated deaths, the tally now stands at 2,518, with ‘all-cause mortality in Norway [being] normal in the past 12 weeks, with the exception of weeks 8 and 9…all-cause mortality…has been within the expected range, with the exception of weeks 43-45 and 47-51 2021’.
As of 27 March, there’s virtually no change in injection uptake: 73% of the entire population received two injections (88% of 16+ and 89% of 18+); 83% of 16-17yo and 54% of 12-15yo received one injection; 43% of 16-17yo received two injections.
As regards ‘boosters’, 53% of the entire population received a third injection; the share is 90% among 65+, 82% for 45+, and 66% for 18+. Among vulnerable groups, 81% of all 18-64yo in high-risk groups received a ‘booster’, as opposed to 73% in moderate risk groups.
Omicron BA.2 surpassed BA.1 in week 6 (mid-February) and now constitutes 93% of all sequenced tissue samples from the past two weeks.
In addition—but this will be discussed in more detail in tomorrow’s dedicated post—there’s now an abnormally late influenza A (H3N2) outbreak going on. Compared to all respiratory illnesses, Covid-19 constitutes 58% of all samples, lower respiratory infections 30%, upper respiratory infections 7%, influenza 5%, and RSV <1% (all data from week 11).
A Pandemic of the ‘Vaccinated’, in Particular Booster Recipients
First up, Fig. 3 (p. 9), which shows the elevated incidences among 75-84yo (the dotted golden line) and 85+ yo (grey line):
Next, Table 6 (p. 11), which tracks overall numbers compares them to the past four weeks.

The data isn’t nice: if you’d add grunnvaksinert (two doses) + mottat 3 doser (boosted) = 4,010 since the beginning of the ‘pandemic’. They’re almost the same numbers, and at the rate of increase, ‘all-cause vaccinated’ will overtake the ‘unvaccinated’ in 1-2 weeks, as a brief look at the same figure from week 9 shows:

Changes in all-cause admissions since week 9 may thus be summarised as followed:
4,287 admissions (week 9) => 4,528 (week 12); difference 241, or +5.6%
1,559 among two-dose recipients => 1,729; diff. 170, or + 10.9%
1,418 among booster recipients => 2,281; diff. 863, or +60.9%
Changes in ICU admissions since week 9:
785 admissions (week 9) => 796 (week 12); difference 9, or +1.4%
170 among two-dose recipients => 177; diff. 7, or + 4%
99 among booster recipients => 135; diff. 36, or +36.4%
Changes in ventilation requirements since week 9:
702 admissions (week 9) => 713 (week 12); difference 11, or +1.6%
150 among two-dose recipients => 156; diff. 6, or + 4%
80 among booster recipients => 106; diff. 26, or +32.5%
Clearly, epidemiological pressure emanates from ‘the vaccinated’, in particular ‘booster’ recipients.
The differences are extremely meaningful, for in the past four weeks alone, they mean that…
…a boosted individual was more than 10X (10.875), and a two-dose recipient was 2X, more likely to be hospitalised for Covid-19 as a main cause compared to an ‘unvaccinated’ individual.
…a boosted individual was more than 20X (20.3125), and a two-dose recipient was almost 3X (2.85) more likely to end up in the ICU for Covid-19 as a main cause compared to an ‘unvaccinated’ individual.
…a boosted individual was 26X (!!!), and a two-dose recipient was 2.5X, more likely to require mechanical ventilation for Covid-19 as a main cause compared to an ‘unvaccinated’ individual.
Also, do take another look at table 6: virtually everyone who ends up in the ICU and/or requiring mechanical ventilation (86-90% or more) has either medium or high underlying risks, i.e., any number of pre-existing conditions, such as diabetes, cardiovascular problems, and the like.
Thus, another question for the government and the Norwegian health authorities: why do you still peddle the notion that these injections actually help at least high-risk groups?
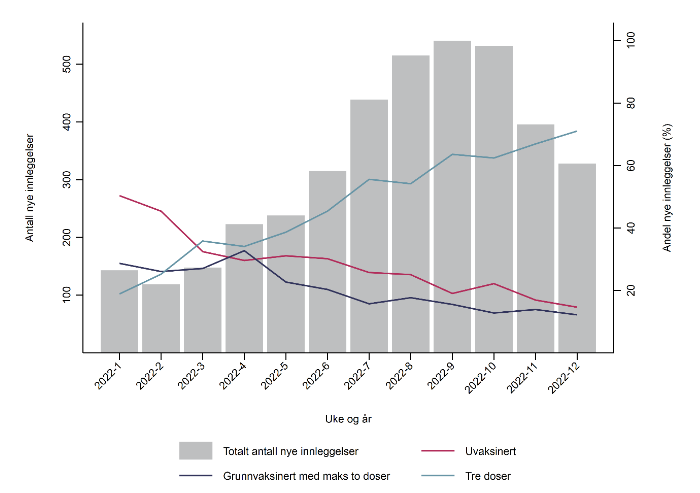
Another way to visualise the above is the below Fig. 4 (p. 12), which gives away the game:
Last Words: Covid-associated Deaths
Here’s Table 8 (p. 16), which shows—almost—everything:

Note, in particular, that for a few weeks now Covid-19 associated deaths among ‘all-cause vaccinated’ exceed those of ‘unvaccinated’. How much has this picture changed, you may ask?

For comparisons, we turn again to the same table from week 9:
Changes in Covid-associated deaths since week 9 may be summarised as follows:
All deaths among ‘unvaccinated’: 605 (week 9) => 662; difference 57, or +9.4%
All deaths among ‘all-cause vaccinated’: 665 (week 9) => 877, diff. 212, or +32.9%
Changes in the past four weeks along
All deaths among ‘unvaccinated’: 59 (week 9) => 68, diff. 9, or +15.2%
All deaths among ‘all-cause vaccinated’: 161 (week 9) => 252, diff. 91, or +56.5%
Stay tuned for tomorrow’s post on how the powers-that-be are struggling to explain this.
Well, at least they separate vaccinated and unvaccinated in the public data, that's not done here as far as I can find. On the other hand, the official line is now "the vaccines are not dangerous or harmful" where it earlier read "the vaccines are safe" - feel free to apply Kremlology as needed.
For Sweden to compare, they haven't stopped counting or presenting data but testing is out since 9th of Februar (if I recall correctly), it is now only done when someone has obvious symptoms.
This page is the gateway to more detailed graphs and charts, you'll have to pick an "entry" depending on your web reader so I can't diect-link to the charts themselves:
[https://www.folkhalsomyndigheten.se/smittskydd-beredskap/utbrott/aktuella-utbrott/covid-19/statistik-och-analyser/bekraftade-fall-i-sverige/] There might be a slight lag when loading the charts, and they are now updated on Thursdays only.
Out of 35 000 tests administered week 12, 17% showed viral being present, down from 20% of tests for week 11, and that's been the trend since the first week of February, where the rate dropped from tens of thousands of cases late January to being in the hundreds just two weeks later. Which I guess is normal for flu season?
Folkhälsomyndigheten (Agency for public health) estimate that 1.4% of the population are carriers.
About 15% to 20% of casualties are unvaccinated, so the majority are those who are double or triple vaccinated, old and have comorbidities. Nothing new about that - but the majority of casualties are now among people living in special housing for elderly or people with disabilities or cognitive handicaps. More than half the deaths for week 11 came from this subset: little to no education, no jobs, no income, minimum welfare and the swedish municipalities typically use old and sometimes condemned buildings to house these people in.
Total number of deaths for the entire Covid-affair stands at 16 245, as confirmed by post-mortem lab testing.
Meanwhile, our politicians are completely ignorant about the variant spreading from Hong Kong via South Korea to Australia. From what Igor Chudov is reporting about Hong Kong, the lethality is much higher than previous Omikron-variants. Want to bet that this time all our authorities decide to again do the exact opposite to what they should do?