
The Calm Before the Child Calls out the Naked Emperor, Pt. 1
News from Life with (under) Covid in Norway: public health bodies introduce a new data tool, which, perhaps counter-intuitively so, points towards massive public policy failures

After ostentatiously getting Covid—which is something I still don’t know for sure: where there’s no doctor, there cannot be a diagnosis—it’s time to address the more serious issues lingering for the past couple of days.
Believe it or not, there has been much change over the weekend, even though its full significance remains yet to be fully understood. While its impact is similarly hard to assess as of today, it’s certainly quite important to learn about these significant developments
This is going to be another two-part series, with this first instalment dealing with the issue of hospitalisation ‘for and with’ Covid, which is the one metric generally touted to support any restrictions on normal life lest the health care system is overwhelmed.
In part 2, which will appear tomorrow, we’ll take a much more granular look at vaccine efficacy, hospitalisation, and deaths ‘of and with’ Covid. If you’d like to read up on this beforehand, you’re re-directed to this pre-print paper by Whittaker et al.
Walking Around Unashamedly Without Clothes
As you, my dear readers, very well know, the Scandinavian governments and their public health authorities publish o.k.-ish Covid data, especially if compared to most (western) counterparts. The main players here were the Institute of Public Health (IPH), which runs a nice, if convoluted, website that offers a shitload of information. (Note that I’ve linked to the Norwegian version, which is more detailed than the English website.)
There were weekly reports, loads of data (but don’t look twice, for the numbers and graphs may be somewhat contradictory), and the like, but despite all the numbers, graphs, and visualisations, there is one metric missing: the relation between all matters Covid vs. all other healthcare-related matters.
To set this piece up properly, here are three such images taken from the section on ‘Statistics about Sars-Cov-2 and Covid-19’ from the IPH’s website, which show the cumulative developments of hospitalisations, ICU admissions, and death ‘with Covid-19 as main cause’, respectively:



Now, this all looks super-transparent (esp. compared with data from, say, the US), but do note that, as nice as these graphs look, they are also useless.
All matters Covid-19 is perhaps the first of its kind where people have stopped using annualised numbers (at this point, I do wonder what that kind of cumulative number of influenza-like illnesses-associated casualties since the Spanish Flu looks like, which serves as an illustration here).
Furthermore, these are all cumulative numbers, which obscure change over time (yes, you can click on the ‘table’ header and then you’ll get daily numbers, but their temporal range is super-short—i.e., some 15 days—which doesn’t allow the casual reader to penetrate the fog of disinformation).
Finally, these numbers don’t relate the burden of ‘Covid-19-the-disease’ to the healthcare system at-large, which is essential to understand the how dangerous Covid-19-the-social-construct is to society-at-large.
Now, I’m not accusing the IPH to intentionally obscure these data. What I am saying is this: in over-emphasising ‘Covid-19-the-disease’, the IPH and its camp followers in the media are running the risk of making mountains out of molehills, figuratively speaking.
Sidenote: if you ever wondered who the people are that work in such public health authorities, I’m glad you asked. It is here—with my ‘unique’ insights into such matters (I worked for a year in the Austrian Foreign Ministry during my Ph.D. work)—that I can offer some helpful guidance. Keep in mind that I bear no ill intentions towards those who may feel insulted by the following two paragraphs: I’m the messenger, hence please don’t shoot me for pointing out the obvious.
Basically, (para-) governmental agencies like the IPH are recruiting its personnel from the bottom rungs of university graduates. Yes, there certainly are differences between governmental agencies, ministries, and the like, but this is tantamount to stating that ‘foreign service’ (which brings with it a number of perks, such as frequent travelling and the like) is more attractive than, say, being in charge of sewage treatment and its environmental impact in rural areas. Now, I’m not saying that the former is actually more important than the latter, but I am saying that the former attracts a different kind of university graduate than the latter.
There are some better positions in agencies like the IPH, but they are reserved for the well-connected among us (here’s looking at you, director Camilla Stoltenberg), but the vast majority of the jobs over at these institutions is actually going to two kinds of individuals: those who fail to make it elsewhere and/or those who are weirdly fanatical about public health and hygiene (here’s looking at you, chief epidemiologist Preben Aavitsland). Yes, those who work there are all highly-credentialled, but they are also the least-capable university graduates, which also serves as an indictment of the decay of western-style ‘higher education’ (but that’s a story for another post).
All told, the main points are these: the people who make decisions are basically political appointees with good connections, and the people who prepare the papers for these decisions are typically fanatics (which is why they rose through the ranks faster than their co-workers). Keep in mind that these basic tenets also characterise all other governmental bodies, national and local, as well as international.
Now, imagine that no-one really paid much attention to you and your work pre-Covid, but for the past two years you were, well, quite a star in terms of public attention. Imagine that the government is now to take back the centre stage by banning the IPH from press conferences. And, finally, imagine further that you are now confronted with numerous inconsistencies in your work of the past two years, which may have been understandable given the enormous pressure that lasted on the IPH (and other such bodies).
Still, don’t expect much sympathy from the media, which will turn on the public health authorities before you could catch your breath. I won’t get into the whole media clown car here, but given their insane levels of bullshit-peddling over the past two years in particular, their ‘natural’ reaction will be this: to deflect from their own shortcomings and failures, everyone else will be blamed, and they’ll start with the IPH.
The Day of Reckoning is Coming Soon
Now, why would I claim that? Well, the ‘secret’ is out—four out of ten hospitalisations are ‘with’, as opposed to ‘for’, Covid-19. Two days ago, Aftenposten reported (paywalled) on the fact that the IPH is—finally—releasing data on the entire co-morbidity issue.
When the government introduced new measures in mid-December, the reason given was that there were more than 300 Covid-related hospitalisations with Covid.
Yet, many of those aren’t actually hospitalised for Covid. Last week [week 2], 40% of Covid admissions were hospitalised for other reasons, with Covid being an incidental observation.
Now, this seemingly innocuous statement reveals that the floodgates have been opened to more realistically assess ‘Covid-19-the-social-construct’. Aftenposten was reporting on the Helsedirektoratet (the supra-ordinate governmental Healthcare Directorate) new online tool that allows individuals to directly assess the relation between all-cause hospitalisations vs. admission for/with Covid.
As of 16 Jan. 2022, the situation looks like this:
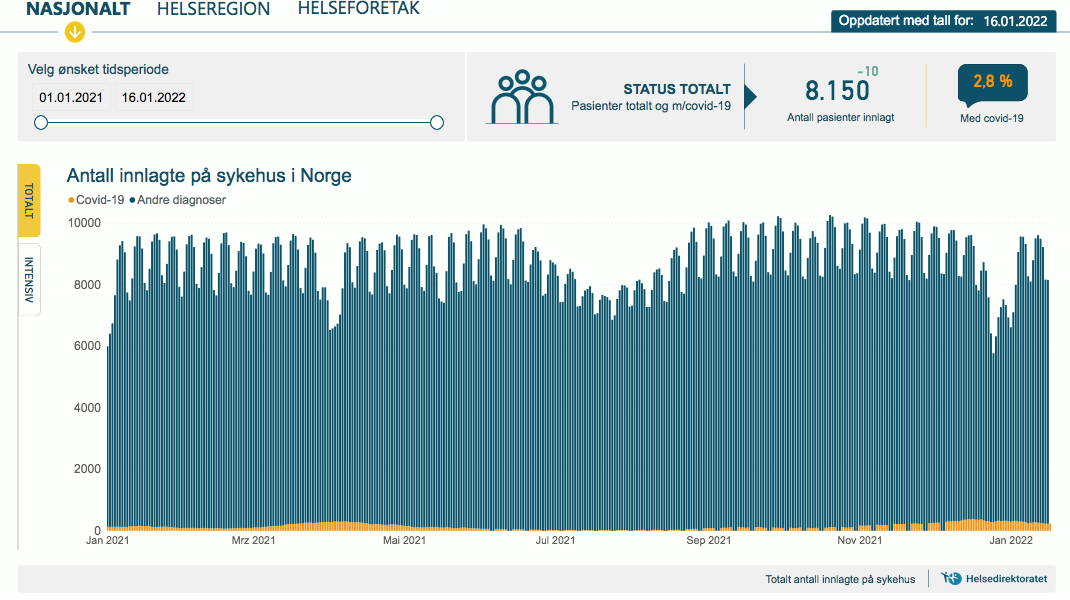
It’s quite different from the situation in Norwegian ICUs: Covid-19 patients clock in at 32.8%.

Now, I don’t mean to be presumptuous, but may I ask a question or two about this:
Governments are now telling everyone that Omicron is mild and that all-cause hospitalisations are way down. This appears to be partially true, as the Norwegian data shows.
At the same time, governments are also peddling the notion that re-openings may proceed because all-cause hospitalisations with or for Omicron are way down. This also appears to be partially true, but this is not borne out by the ICU data.
Speaking about the ICU data, well, if the above-mentioned Aftenposten piece is correct, then 40% of these patients would be in the ICU for other causes. In other words: the above visualisation should show ICU admission with or for Covid at slightly below 20% of the total.
Keep in mind that ICU occupancy is actually a subset of all-cause hospitalisation. This means that even though the share of Covid-related ICU occupancy (with due consideration of the above reservations, I’d hasten to add) must be seen in light of the overall pressures resting on the healthcare system as a whole.
What’s the rub, though?
Be that as it may, these data show that Covid-19 is not only very much subject to risk stratification by age, but that a more granular look is warranted, if not called for.
Keep in mind that, according to the most recent data provided by the Helsedirektoratet, as of 16 Jan. 2021, there were 8,150 hospitalised patients in Norway of whom 2.8% (228 or 229) were in hospitals for or with Covid-19. There were 261 patients in the country’s ICUs, of whom 32% (83 or 84) were there for or with Covid-19.
If we now apply the same criteria outlined above (40% of patients are actually admitted with, as opposed for, Covid-19), these numbers shrink to 91 or 92 all-cause hospitalisations and 33 or 34 ICU admissions for Covid-19.
Let that sink in for a moment.
And now let’s consider the implications
I’m not claiming that these aren’t tragical incidences without much suffering and sorrow.
I do wish to point out that these numbers, to me at least, do not warrant any of the heavy-handed intrusions into everyone’s life whatsoever.
Furthermore, this is compelling evidence that what we’ve been told from the outset—remember the ‘two weeks to flatten the curve’ from March 2020?—was a darned lie, to put this mildly.
At this point, there’s but one essential question: was there ever an emergency that justified these Covid-19 measures?
Finally, for this post, what about the self-inflicted loss of trust in public authorities? It’s hard to imagine (although not entirely impossible) that—even Scandinavians—will just meekly accept this gigantic series of failures wrapped in lies to obscure the more embarrassing public policy mistakes, which were all covered up by a subservient and, frankly, irresponsible legacy media.
At the end of part 1, let me ask you this, then: anger is a well-known human emotion, and it is also a very destructive state of mind. Personally, I don’t object to it, but to use anger productively, it’s necessary to direct (legitimate) anger at the right person(s) at the right time and under the right circumstances.
In my reading, we’ve (almost) arrived at this point.
"...where there’s no doctor, there cannot be a diagnosis..."
R U sure?
In Queensland, Australia, you are allowed to doctor yourself:
"If you're a healthy young adult, particularly if you've been vaccinated and you have something that looks like a common cold or flu, assume it's COVID, stay at home," he said.
https://www.abc.net.au/news/2022-01-05/covid-symptoms-stay-home-testing-queues/100738206
Well, yes and no.
The numbers seem reduced for total hospitalizations, but ICUs numbers are terrible. Please remember that last 30 years of health policy has been to increase efficiency of the health system. That means that all hospital units should run close to maximum capacity, including ICUs. So if in a normal winter you are running around max capacity, 647 according to Guldvog today in VG, and you throw a couple of hundreds on top of it, people are going to start dying in droves. Whose failure is that one is left for debate. And that 647 is pulling all available resources at it, so I doubt it is even reasonable.
For a couple of anecdotes:
A friend of mine gets heart operated around April 2009 in riksen, placed in pediatric ICU because there was no room in adults ICU.
That ICU doctor in vg complaining about the heavy toll on young vulnerable person's, many dead by overdose like her son, telling that the ICU she has worked in for almost two decades is collapsed every winter.
In those conditions running fully open is a disaster.