
'Highlights from the sixth ESCMID Conference on Vaccines'
Reporting™ in The Lancet's current issue (Nov. 2025) on one of the latest poison/death juice pushers and their promises™ of 'lifelong vaccination'

As indicated in yesterday’s posting—which was a serious mind-f*** in and of itself—I told you that I’d be following up with some more paywalled content from The Lancet’s current (Nov. 2025) issue; click on the linked content below to read the editorial (plus my snark):

Today, we’ll look at what happens when a vaxx-nik attends a vaccinology™ conference and reports™ on what she experienced.
Emphases and [snark] mine, as are the bottom lines. *enjoy*
Highlights from the sixth ESCMID Conference on Vaccines
The sixth European Society of Clinical Microbiology and Infectious Diseases Conference on Vaccines took place in Lisbon, Portugal, from Sept 10 to Sept 13, 2025.
By Claire Lenahan, The Lancet Infectious Diseases, Volume 25, Issue 11, e631 [source (paywalled)]
The European Society of Clinical Microbiology and Infectious Diseases (ESCMID) hosted its sixth vaccine-related conference in Lisbon, Portugal, in September [even link], with an intentionally broad focus on the full vaccine pipeline, from vaccine development to programme implementation. The 4-day conference opened with two introductory sessions presented by Alessandro Sette (La Jolla Institute for Immunology, CA, USA) and Ioanna Papadatou (National and Kapodistrian University of Athens, Greece) on different mechanisms of immune activation following vaccination and correlates of protection (CoPs) for vaccine-induced immune responses. Both sessions emphasised the promise of investigating different immune responses for vaccine development and the need to diversify CoPs beyond antibodies (including T-cell, memory B-cell, and mucosal responses) [which tells you what Big Pharma hasn’t done so far]. In a presentation on new developments in vaccine administration routes (including an intranasal pertussis vaccine), Marien de Jonge (Radboud University, Netherlands) also commented on this challenge, noting that novel vaccines will probably require different CoPs for future licensure [so, keep an eye on Big Pharma’s 10-Q forms and a whole host of ‘novel’ licensure shenanigans applications].
Use of controlled human infection models (CHIMs), which involve deliberately exposing consenting participants to infectious diseases, was another popular topic at the conference [ask yourself: what could go wrong?] Meta Roestenberg (Leiden University Medical Center, Netherlands) gave a presentation on the importance of CHIM studies for vaccine research and development, highlighting their common use in malaria vaccine design [I’ll interrupt the flow here to highlight how such trials™ are done—in Africa:

Here’s from that piece I wrote last year in summer:
[Here follows an info box that explains something about the injections: the product used in Cameroon goes by the name RTS S, and it is also known as Moquirix; it is manufactured by GlaxoSmithKline in collaboration with PATH, a self-declared organisation dedicated to achieving ‘vaccine equity’, is a ‘charitable’ institution (as per US law) financed overwhelmingly by ‘foundations’ and the US gov’t, and their list of donors (p. 26-29) list, well, a ton of ‘usual suspects’.
And then there’s the Matrix-M product developed—much like the AstraZeneca Covid gene therapy product—by the U of Oxford (AZ is one of PATH’s donors, by the way). Reference is made to several studies and trials, with the results summarised as follows:
Both products were ‘repeatedly tested’ in Ghana, Malawi, and Kenya, ‘resulting in a -13% change in death rates’, achieved albeit ‘irrespective of malaria or other diseases being the cause of death’.
The information box derives information from GAVI, the Gates-funded pro-jab diehards, ‘with generous support from Norway’, the infobox concludes.
Note that GSK, or GlaxoSmithKline is a seemingly proud sponsor of the ECSMID conference in Lisbon, Portugal, this year (via the prospectus: see the program at p. 4 and the particulars about the breakfast—6,000 euros excl. VAT—and lunch sessions—12,000 euros excl. VAT— sponsored by GSK at p. 10). AstraZeneca—of Covid poison/death juice infamy—also sponsors the ECSMID conference, by the way; and now—back to Claire Lenahan’s reporting™]
CHIMs were essential to the development of the WHO-recommended malaria vaccines RTS,S and R21 [now you know why I interrupted the flow], which have been rolled out across Africa, and Roestenberg commented that no malaria vaccine studies make it to late-stage trials anymore without the use of CHIMs. [line break added]
Marco Cavaleri (European Medicines Agency) included CHIMs in his presentation on different licensure pathways for vaccines for emerging infectious diseases [note that ‘emerging infectious diseases’ most likely includes so-called gain-of-function research™, otherwise known as bioweapon warfare technically prohibited under int’l law but, hey, who cares], and Deborah Williamson (University of St Andrews, UK) discussed the use of challenge studies for gonorrhoea vaccine development in a presentation on recent advances in vaccines against gonococci, chlamydia, and syphilis [surely the most pressing concerns; shall we thrown in MonkeyPox™ shots for sexually prolific homosexuals, too? In case you wish to have your mind blown, consider the case of the shady D.C.-based ‘Alliance for Biosecurity’ that appears to be in charge *ahem* of the MPox hoax:

Turns out, though, that such vaccinology™ conferences and these outfits are sponsored by the very same (bad faith) actors in Big Pharma: go figure]. Williamson presented a systematic Neisseria gonorrhoeae challenge strain selection strategy, which was recently published in The Lancet Microbiology.
In a meet-the-expert session [no irony here] on the future of real-world evidence, Sabrina Bacci (European Centre for Disease Prevention and Control) emphasised the importance of post-authorisation studies of vaccine effectiveness [did I mention that ‘vaxx effictiveness’ is a hoax, too? The give-away is the comparison of any injection vs. a saline placebo, which—even legacy media admits—has never been done1]. Julie Rowbotham (UK Health Security Agency, UK) described how health economic and transmission models can also be used to help evaluate vaccine effectiveness in a presentation on the PrIMAVeRa consortium. Models can be used to simulate both disease transmission and different intervention strategies [what happens if when these models turn out to be wrong-to-misleading? Cf. the Church of Climatology™, if in doubt, I suppose], including those aimed at addressing antimicrobial resistance (AMR). Rowbotham highlighted that vaccines are mostly missing from national plans to address AMR [perhaps because viruses and antibiotics rarely go hand in had because…viruses can’t be treated with antibiotics? I mean, that’s their science™, not mine] and few mathematical models address the impact of vaccination on antibiotic resistance. PrIMAVeRa is developing a modelling dashboard for Europe, which will hopefully identify data gaps for future modelling studies [I’m somewhat intrigued to check out that one…] .
Adult vaccination programmes were key to many of the discussions around vaccine policy and practice. In a symposium on broader perspectives on adult immunisation beyond pregnancy and old age, Pier Luigi Lopalco (University of Salento, Italy) made the argument for maintaining routine vaccinations into adulthood by including them in routine health checks (especially those offered by workplaces) and increasing their accessibility at pharmacies and travel health clinics [now you see the connection with the EU Covid Passport shitshow that the WHO took over in 2023, right? Right. Find out ‘more’ here:
But there was, of course, more to the ECSMID conference.]
The conference saw presentations on vaccines currently in development for a wide range of infectious diseases, including respiratory, gastrointestinal, vector-borne, and sexually transmitted infections. With so many vaccines in the pipeline (and concerns voiced around vaccine hesitancy), the need for harmonised vaccine approval and development of combination vaccines (which reduce the number of necessary vaccine administrations, benefitting both vaccine recipients and health-care workers) was also discussed [I’m sure you assholes had a ball]. Francisca Mutapi (University of Edinburgh, UK) spoke about her quest for an effective schistosomiasis2 vaccine [check out the footnote: there are existing treatment options at relatively low costs (Merck said they’d donate 250m treatments in 2012) and ask yourself: why the need™ for an injectable product? We all know the answer] and emphasised that differing licensure pathways among African countries would make any such vaccine that much harder to practically implement [here’s a pro tip: declare a PHEIC (public health emergence of international concern), disregard existing treatments, and mandate injections: you’re welcome]. Hanna M Nohynek (Finnish Institute for Health and Welfare, Finland) gave a presentation on the future of combination vaccines against respiratory viruses and informed conference attendees that combination vaccines were on the agenda for the September, 2025, meeting of the WHO Strategic Advisory Group of Experts on Immunization. Nohynek closed the conference alongside Raquel Guiomar (National Institute of Health, Portugal) in a session on avian influenza, offering insights into Finland’s vaccine response to avian influenza outbreaks in the fur industry [ah, bird flu; time to highlight two more pieces I wrote some time ago:
And here’s some ‘old news’ from 2013 when we could still talk about the fact that ‘bird flu’ is the result of Frankenstein-esque gain-of-function research™:
Thank me later].
Bottom Lines
I have questions. Many. You know, such as, for instance, who funded that conference? Here’s the organisers’ prospectus, and I’m providing the below screenshot for educational purposes only:
Inside that prospectus, you can also learn the answers to the question ‘why sponsor?’ (at p. 7):
Increase your global visibility! ESCMID provides many opportunities for your company to increase visibility and showcase your products messages and benefits [sponsoring with benefits, anyone?] while supporting the conference activities
The ESCMID mission is to improve the diagnosis, treatment and prevention of infection-related diseases. This is achieved by promoting and supporting research, education, training, and good medical practice. With its yearly congress and different conferences throughout the year it pursues this objective
ESCMID offers marketing and sponsorship opportunities to create and build brand awareness
It is a unique opportunity to network with colleagues, build relationships, and generate leads from around 400 attendees in just a few days.
Near the top of the many things I’ll never tire to point out about academia is—the ludicrously small amounts of money it takes to co-opt academics:
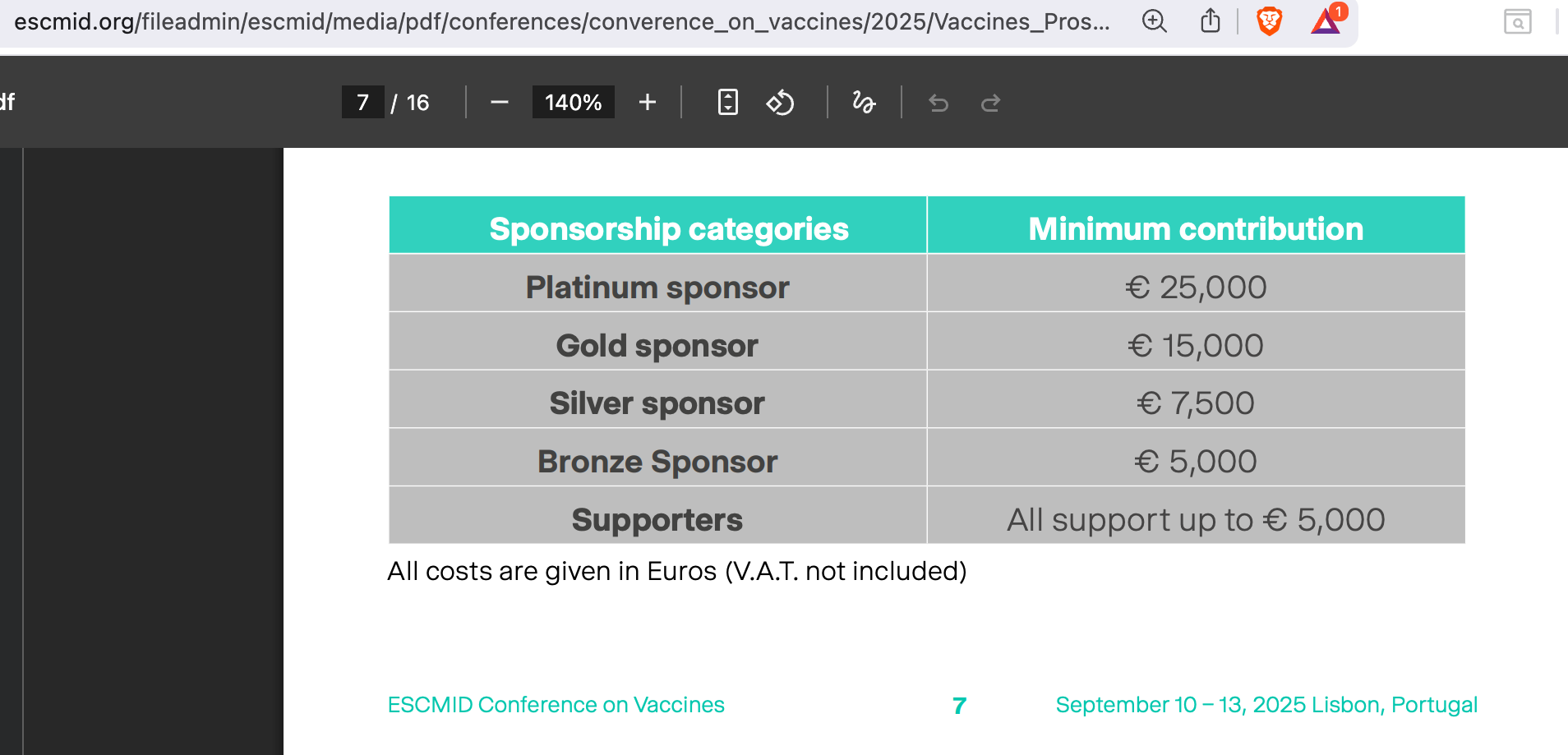
Throw in two graduate students handing out ball pens, candy, and flyers, as well as 1-2 company PR people plus the platinum fee, I suppose that all comes at way less than 100K: pocket change for the likes of AZ or Pfizer.
The main issue, I’d note to close out this heavily annotated shitshow is this:
We’ve long-since departed reality-as-is in regards to geopolitics, finance, and price discovery via market places (as the gov’ts and central banks, in cahoots with Big Finance have been manipulating price signals for decades).
This results in virtually everything being mis-priced, with a substantial correction around the corner one way or another. In macro-economic terms, such a correction is long overdue, and the one thing that permits gov’ts to kick that can of worms down the road a tad longer is—World War III.
As regards (public) healthcare™, well, I suppose that if you’re still believing the cultists peddling this shit known as vaccinology™, well, there’s very little I can do to make you change your mind. Go and get a few more combination shots against Flurona or whatever.
If you read the above and leave with the sentiment that, well, all is exactly as it should be, you’re equally well beyond.
If, however, you read this and go, well, there’s so much abuse going on and I should tell e.g. my ageing parents or children-in-law who’re about to welcome their first child, please do.
DO IT *now*, for you may save countless lives.
Here’s from a randomly picked tell-tale feature in the BBC, which I’m citing as an example (source; archived):
The top US health department plans to require placebo testing for all vaccines in an effort to offer “straightforward” public health information, but experts say such testing could limit availability and raise ethical concerns.
In a statement first given to the Washington Post, the Department of Health and Human Services (HHS) said this week, “All new vaccines will undergo safety testing in placebo-controlled trials prior to licensure — a radical departure from past practices”…
Peter Lurie, a former official with the Food and Drug Administration (FDA), said “it’s hard to tell exactly what is being proposed.”
“But, broadly, if they mean that every modification to an existing vaccine would require a new placebo-controlled trial, they are treading in ethically dubious territory and likely to deny Americans life-saving vaccines at some point.”
Don’t fall for this nonsense; so far, most comparisons of a new injectable product were other such products, e.g., older versions or the like; there are no such randomised, placebo-controlled studies, hence the panic mode over at regulators™ and Big Pharma alike. Don’t take my word for it, here’s the BBC’s:
An HHS spokesperson told the BBC in a statement that health secretary Robert F Kennedy Jr’s goal of “radical transparency” means being “honest and straightforward about what we know — and what we don’t know — about medical products, including vaccines”.
The statement said none of the childhood vaccines recommended in the US - except [sic] the Covid shot - had undergone “inert placebo” testing, meaning “we know very little about the actual risk profiles of these products”.
But public health experts say the statement is misleading, as childhood vaccinations, including ones for Hepatitis A and B, rotavirus, polio and the mumps, were all initially tested against a placebo. In fact, all new immunizations already go through the trials - a type of random testing where one test group receives the immunization, and the other gets a placebo, like a saline shot [maybe so, but the original injectable products have all been replaced, so we’re also talking about the human trial equivalent of data splice in regards to data visualisations of the same thing (e.g., CO2 measurements) using different sensors over time—and this is explicitly admitted in the next sentence].
But newer versions of the shots may not go through the same process, because it is considered unethical to withhold a shot known to be safe from a particular group, and because the shot is only being tweaked in a minor way [which we don’t know shit about], vaccine experts said.
The coronavirus shot, for example, already has gone through rigorous safety testing, said Paul Offit, director of the Vaccine Education Center at Children’s Hospital of Philadelphia [of course he would say that: 8 mice were sacrificed, to say nothing about tens of thousands entries in vaccine safety monitoring systems, such as VAERS or EudraVigilance, but, hey, vaxx pushers cannot be blamed for any of that, eh?].
I’ll go and vomit now.
This is another classic example of ‘WTF injections?’. Here are the basics of this problem™ via Wikipedia, which ‘splains that schistosomiasis is
a neglected tropical disease caused by parasitic flatworms called schistosomes.[5] It affects both humans and animals. It affects the urinary tract or the intestines.[5] Symptoms include abdominal pain, diarrhea, bloody stool, or blood in the urine.[5] Those who have been infected for a long time may experience liver damage, kidney failure, infertility, or bladder cancer.[5] In children, schistosomiasis may cause poor growth and learning difficulties.[5] Schistosomiasis belongs to the group of helminth infections.[10]…
Methods of preventing the disease include improving access to clean water and reducing the number of snails.[5] In areas where the disease is common, the medication praziquantel may be given once a year to the entire group.[5] This is done to decrease the number of people infected, and consequently, the spread of the disease.[5] Praziquantel is also the treatment recommended by the World Health Organization (WHO) for those who are known to be infected.[5]
The disease is especially common among children in underdeveloped and developing countries because they are more likely to play in contaminated water.[5] Schistosomiasis is also common among women, who may have greater exposure through daily chores that involve water, such as washing clothes and fetching water.[11] Other high-risk groups include farmers, fishermen, and people using unclean water during daily living.[5]
So, we have a cheap and apparently working treatment options:
Two drugs, praziquantel and oxamniquine, are available for the treatment of schistosomiasis.[63] They are considered equivalent in relation to efficacy against S. mansoni and safety.[64]…Because of praziquantel’s lower cost per treatment, and oxaminiquine’s lack of efficacy against the urogenital form of the disease caused by S. haematobium, in general praziquantel is considered the first option for treatment.[66] Praziquantel can be safely used in pregnant women and young children.[26] The treatment objective is to cure the disease and prevent the progression of the acute to chronic form of the disease. All cases of suspected schistosomiasis should be treated regardless of presentation because the adult parasite can live in the host for years.[67]
Schistosomiasis is treatable by taking a single dose of the drug praziquantel by mouth annually.[68]
Here’s the Mayo Clinic’s information page; according to this website, product costs in the US are US$60-100, though the manufacturer (Merck) announced, back in 2012, to donate 250m treatments to contribute to lessen the burden of disease.
Why the surely more expensive-per-unit vaccine? Well, we both know the answer…
Just today I saw a horrific poster at a small train station in Austria with what I thought was an anti-torture message. But then I saw “GSK” written on it and figure out with my mediocre German it was a demand to get “vaccinated” for shingles at once, lest you suffer too. I’m sure shingles can be quite bad, but my grandfather got it after being vaccinated against it! In the US a decade ago. And he had had chickenpox like everyone else as a child.
Back in Seattle where the Gates Foundation rules supreme, we are constantly asked/reminded/nudged about “updating” our vaccines at every single appointment. Even at a follow-up with a shoulder injury! I was glad to get my shoulder taken care of back here in Austria later, because the healthcare workers actually spent all of their time on my shoulder, not vaccines and going through a transgender checklist with me. I think with my doctors in Seattle they get paid between $40-100 for each vaccine they administer, although the documentation on that was unclear. Money makes the world go round. That conference in Lisbon is a pretty good bargain for them all things considered.