


Covid in Norway: Public Health Officialdom 'splains' Excess Mortality by Monkeying w/Data
A detailed look at how the Norwegian authorities are gaslighting everyone who bothers to take a closer look--but are quite likely deluding themselves even more

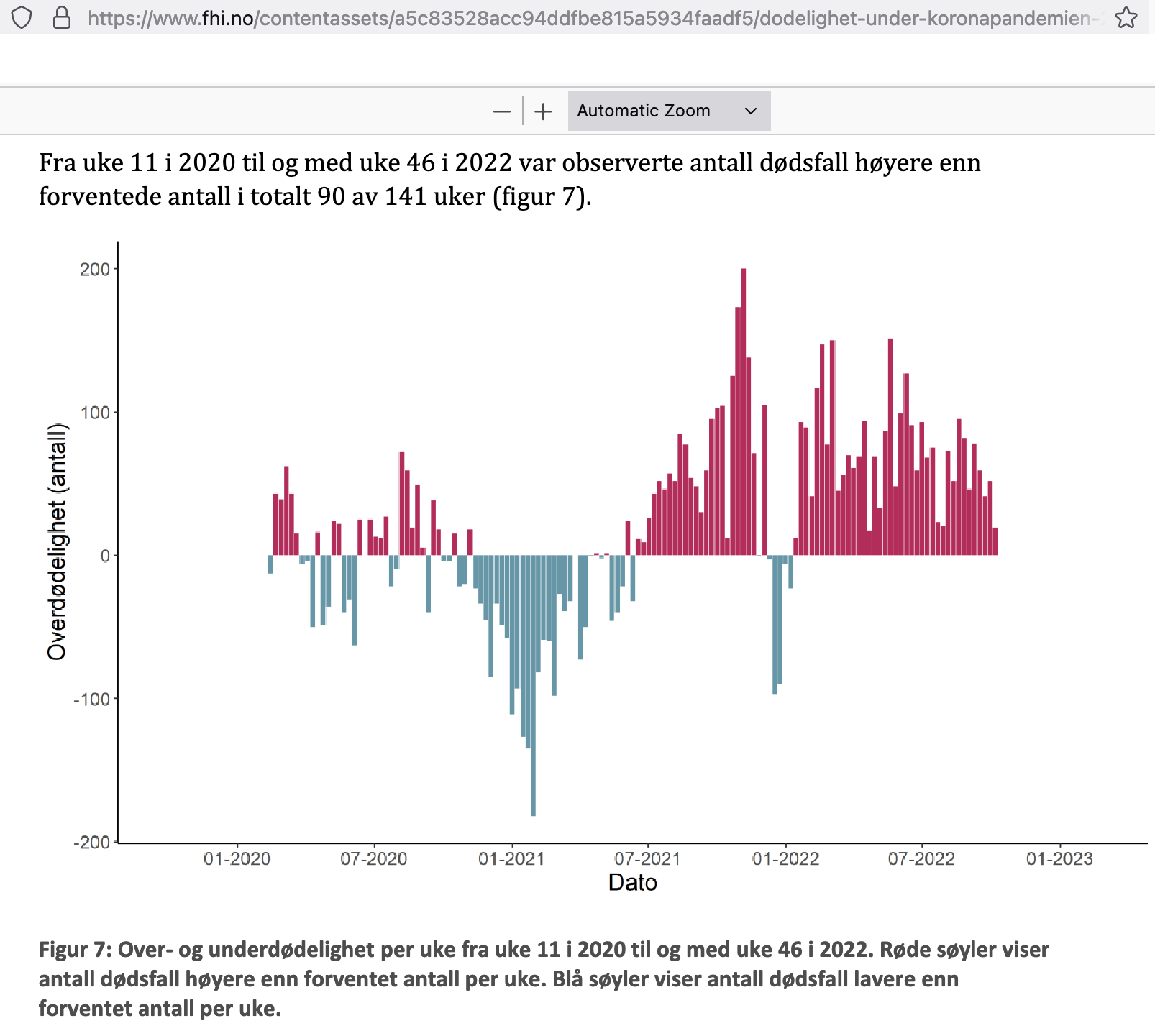
This is a follow-up posting to yesterday’s exposé about the official mortality numbers—7% higher than expected in 2022 through week 46—presented a week ago by the Norwegian Institute of Public Health (IPH). Please click here for that posting.
While yesterday’s post sought to provide the proper context, today, we’ll look at the report itself. Entitled, ‘Mortality in Norway during the Corona Pandemic, 2020 to Autumn 2022’, we’ll be looking at the 34 page-strong memo (notat) authored by the public health officials over at the IPH. Click here if you like to see the news item on their website announcing the main findings.
Preliminary Commentary
This memo seeks to provide an overview of mortality associated with, and during, the Coronavirus episode in Norway; as such, it’s certainly a topic that warrants attention, in particular as persistently elevated levels of excess mortality cast their shadows on the eternally spotless minds of public health officialdom. Background on these notions via:

It has long been a staple of conventional wisdom to consider the Nordic countries as something approximating a ‘gold standard’ of good governance, public trust in state institutions, and social cohesion.
Ever since I began posting about Covid in Norway (if you’re new to my Substack, please use these words in the search function), I have sought to call out the many flaws in Norway’s public health policies; I haven’t done that to gloat about it—after all, I live here and I wouldn’t stand to benefit from it—but to ‘keep the receipts’, thereby contributing to holding officials and decision-makers accountable.
Just last week I was in a video call with one of Austria’s more notorious anti-mandate physicians, Dr. Martin Sprenger, who, truth be told, is among the more courageous doctors of the land. Still, he too appeared reluctant to voice an opinion as to why there aren’t more doctors speaking up, even though I pressed him on the issue.
We’re not even close to that level of ‘notoriety’ here in Norway, though, hence the below chronicle of questionable conduct is all the more appalling. I bring this up because Dr. Sprenger asserted, although without evidence (and I quickly contradicted his assertion), that ‘[he] can’t believe the Scandinavians would be dishonest about all matters Covid’.
Well, ladies and gentlemen, here is further evidence of the more recent vintage (and if your taste desires more aged vintage gaslighting, please venture over to this spring posting).
About That Norwegian Mortality Memo…
It opens quite strongly, with the IPH stating their intent (all emphases here and in the following are mine):
We show differences between age groups, gender, and counties [fylke, akin to states in the US context, but keep in mind that Norway isn’t a federal state], as well as developments in large groups of causes of death and deaths related to Covid-19. We also calculate whether there has been an excess of mortality compared to previous years. We do this by comparing mortality in the pandemic years with expected mortality based on trends in mortality development and seasonal variations in the five years before the pandemic (2015-19), as well as population growth and an increasing proportion of elderly people.
Sounds reasonable enough, eh? Do keep in mind—much like with the Swiss ‘study’ I discussed two days ago—that despite a wealth of variables, the one that would arguably matter most, injection status, is most conspicuously absent.
While any reasonable individual interested in objectively true observations may now, and justifiably so, cast aside this particular memo while claiming that it wouldn’t make much sense to investigate ‘whether there has been an excess of mortality’, let’s nonetheless take a couple of closer looks.
I do realise that this is particularly useless as the memo has been published already and no change in policy appears to be in the offing, but it is nonetheless important to pay attention to these matters, if only to keep the receipts for what looks to me increasingly erratic, transparently ill-intentioned behaviour that has nothing to do with ‘public health’, and, yes, I still haven’t lost my confidence (hope) in any of the leading individuals’ personal accountability for these massive policy failures.
As IPH Director Camilla Stoltenberg explained,
The calculations show excess mortality in 2022. Most of the excess mortality is due to deaths related to Covid-19.
Strange, eh? In a highly vaccinated country. Doesn’t look like we need any other study on ‘vaccine efficacy’, we could just look at mortality associated with Covid-19 as a helpful proxy of ‘real-world’ qualities to determine whether or not these modRNA injections actually, well, reduce the risk of severe disease and/or death.
Here’s how the IPH concludes its ‘main findings’ in that memo (p. 3):
It is still too early to conclude how Covid-19 has changed mortality in the Norwegian population. Observations over longer periods of time are needed before we can distinguish between the expected increase in mortality and temporary or permanent changes in mortality due to the Coronavirus. It is therefore important to continue with ongoing monitoring and in-depth analysis of mortality and causes of death.
Note the conspicuously absent term ‘the vaccine’ and its derivatives.
Speaking of terminology, and keeping in line with the age-old adage of ‘fake it til you make it’, there’s even a set of definitions (p. 5, Italics are emphases in the original, Bold refers to my emphases), which holds the following:
Causes of death are recorded using the International Classification of Diseases and Related Health Problems (ICD-10). For each death, one underlying cause of death must be selected, which can simply be said to be the most important cause of death. Other causes of death are considered contributing causes of death. This text describes Covid-19 associated deaths. It includes both deaths where Covid-19 is registered as the underlying cause of death, and as a contributing cause of death. For the selection of the underlying cause of death, the WHO has given the Covid-19 codes the same weighting as other serious infectious diseases (e.g., influenza). Covid-19 is thus often selected as the underlying cause of death.
So, what this means, to my mind, is that we could stop reading now as the newly invented category of ‘Covid-19 associated deaths’ is something of a composite that conflates dying of Covid with dying with Covid.
Given these preliminaries, it’s easy to use ‘real’, or ‘true’, data inputs as the results will inevitably reproduce any biases fed into these kinds of ‘analysis’.
Obfuscation by the Book
On p. 7, we’ll see the ICD codes for Covid-related deaths:
2) Pandemic-related mortality. We have carried out separate analyses of:
Covid-19-associated deaths (ICD-10 diagnosis code U07.1, U07.2, U09.9, and U10.9)
deaths related to corona vaccination (ICD-10 diagnosis code U12.9)
3) Other cause-specific analyses. In the cause-specific analyses, the causes of death are grouped into the following categories for underlying causes of death:
cancer (ICD-10 diagnosis code C00-C97)
cardiovascular diseases (ICD-10 diagnosis code I00-I99)
lung diseases without covid-19 (ICD-10 diagnosis code J00-J99)
dementia (ICD-10 diagnosis code F01, F03, G30)
Covid-19 (ICD-10 diagnosis code U07.1, U07.2, U09.9 and U10.9)
Just keep in mind that whatever ‘separate’ causes of dying of, or with, Covid-19, they’re all conflated in the final analysis. Talk about exercises in futility, to say nothing about intellectual dishonesty.
Still, here’s how the Norwegian public health officials, aided and abetted by legacy media stooges, downplay the rate of excess mortality:

See the sleight of hand? They 7% excess mortality they cite is the ‘standardised’ rate per 100,000 inhabitants, as opposed to the overall share, which is 10.5%.
Injections Protect the Elderly, Eh?
Moving on to Tab. 2, we can clearly see that whatever Covid was (is), it is clearly affecting the elderly in a very disproportionate sense, with the age brackets from 70 upwards seeing overall increases in mortality between 8.1-21.5%:

There’s a lot more in terms of graphs, tables, and the like (sex, county/fylke), but there’s no breakdown based on injection uptake. We do know that, according to chief epidemiologist Preben Aavitsland, public health officials
know exactly how many people have been vaccinated with each dose and at what time, we do not know how many have undergone infection
Why not include this information in a report on Corona-related excess mortality?
Speaking of Injections and Death
There’s an entire section—actually half a page of text—on this subject matter (pp. 21-2), which is worth quoting in full:
As of 22 November 2022, the Norwegian Medicines Agency had received 268 reports of deaths as a suspected side effect of one of the corona vaccines. Some of the deaths have occurred in temporal connection with vaccination, while other reports are due to deaths from Covid-19 in fully vaccinated individuals several months after the last dose.
In the Cause of Death Register, the [ICD] code ‘U12.9 Side effect caused by Covid-19 vaccine’ is registered as the underlying or contributing cause of death for 51 people [see the sleight of hand: again, people die of the jab or after having been jabbed]. The median age at death for these 51 people was 82 years. Of these 51, there were also 20 deaths reported as a suspected side effect to the pharmaceutical authorities. A closer review of the 51 deaths reported as a vaccine side effect reveals that most have had other life-threatening comorbidities at the time of death that are not related to vaccination [well, wasn’t the injection supposed to protect the vulnerable?].
By the end of November 2022, 4,347,816 people in the Norwegian population had received one or more doses of Covid vaccine. Of these, 67,992 are registered as dead regardless of cause of death and time period since vaccination. The median age at death for these was 83 years. In comparison, the median age at death for all deaths in both 2018 and 2019 was 82 years. In an in-depth research study, the Norwegian Institute of Public Health has investigated the occurrence of deaths shortly after vaccination, regardless of the stated cause of death, among individuals who were 70 years of age and older and who received the vaccine between December 2020 and March 2021 (Lopez-Doriga Ruiz et al., 2022). This analysis showed a reduced mortality among the vaccinated compared to the unvaccinated both in elderly people living at home and elderly people in nursing homes.
Apart from the disingenuity of presenting these notions, here’s what I find particularly dishonest: at first sight, the final paragraph would suggest that, while there are concerns about the safety (harm) from these Covid injectable products, public health officials across two agencies (the IPH and the Norwegian Medicines Agency) are ‘on it’. They did an in-depth study and concluded that, while certainly things aren’t as fine and dandy as they should be, all is well.
But.
Here’s the full reference to the cited study by Lopez-Doriga Ruiz et al:
‘Short-term safety of COVID-19 mRNA vaccines with respect to all-cause mortality in the older population in Norway’, Vaccine (2022), pub. 7 Nov; doi: 10.1016/j.vaccine.2022.10.085.
If you click on that link, you can learn about a ‘nationwide cohort study’ that included close to 700K individuals. You read on, though, to learn of the following results:
Between December 27, 2020, and March 31, 2021, 420,771 older individuals (61.1%) were vaccinated against COVID-19. The Kaplan-Meier estimates based on the matched study sample showed a small absolute risk difference in all-cause mortality between vaccinated and unvaccinated individuals, with a lower mortality in the vaccinated group (overall HR 0.28 [95% CI: 0.24-0.31]). Similar results were obtained in analyses stratified by use of health services and age group.
Yes, you read that correctly: data from the first quarter of 2021—that is, from two (!) years ago—is presented as having any relation whatsoever on the above ‘discussion’ of excess mortality and the modRNA injections.
This is quite a bit away from ‘good scientific practice’ to be observed by everyone who works in research, at universities, or public health. To me, this is about as relevant to the current debates on excess mortality as a child’s pre-K ‘grades’ are predictors of later high school achievement. Sure, there may be an overlap or the like, but it’s quite unlikely to bear much, if any, relevance. I mean, c’mon, man…
Here's that paper’s conclusion:
We found no evidence of increased short-term mortality among vaccinated individuals in the older population after matching on sociodemographic and clinical characteristics affecting vaccination and mortality.
And here, as a reminder, is how the IPH frames this in its current ‘report’:
In an in-depth research study, the Norwegian Institute of Public Health has investigated the occurrence of deaths shortly after vaccination [that] showed a reduced mortality among the vaccinated compared to the unvaccinated both in elderly people living at home and elderly people in nursing homes.
Spot the difference?
Here’s a little help:

Bottom Lines
Call me a cynic, but this isn’t even bad judgement or a regrettable oversight.
To me, this reeks of malfeasance, ill intent, and stinks to high heavens due to the amount of ass-covering.
In other words, that memo is another pile of junk.
Its primary purpose is to absolve public health officials from their responsibilities.
Let’s not let them get away with it.
The one relevant question here seems to be: if Norway, which hasn’t had any mandates since Feb. 2022, is faring about as badly as other countries that kept (keep) mandates (here’s looking at you, Austria), the most helpful issue to ponder would be:
It’s not the mandates, it’s the injections, stupid!
How many more people will need to suffer before this is addressed?
Is there a detailed table of causes of death by ICD-10 code for Norway? I haven't found one, but it would be interesting (I mapped the German data to Joel Smalley's English data, and it is interesting to observe similarities and differences).