


Covid in Norway: Public Health Officials Answer my Questions (sort of)
Join me on my Quixotic adventure as the IPH seeks to rewrite 'pandemic' history and fails to really answer anything, BUT at least I've got their attention now (and Aavitsland‘s email address)

Editorial remark: this is a long posting, please read it on the app or online.
Well, this is also quite unplanned, as well as unexpected. You see, I was putting together a long-form essay over at tkp.at (it’s in German, and if you can read it: here), which is basically a somewhat polished version of this week’s postings on the subject matter—with one big exception: I’ve gotten answers from the Norwegian Institute of Public Health.
So, let’s backtrack a bit, shall we?
Step 1: the not-so-secretly ‘updated’ risk assessment
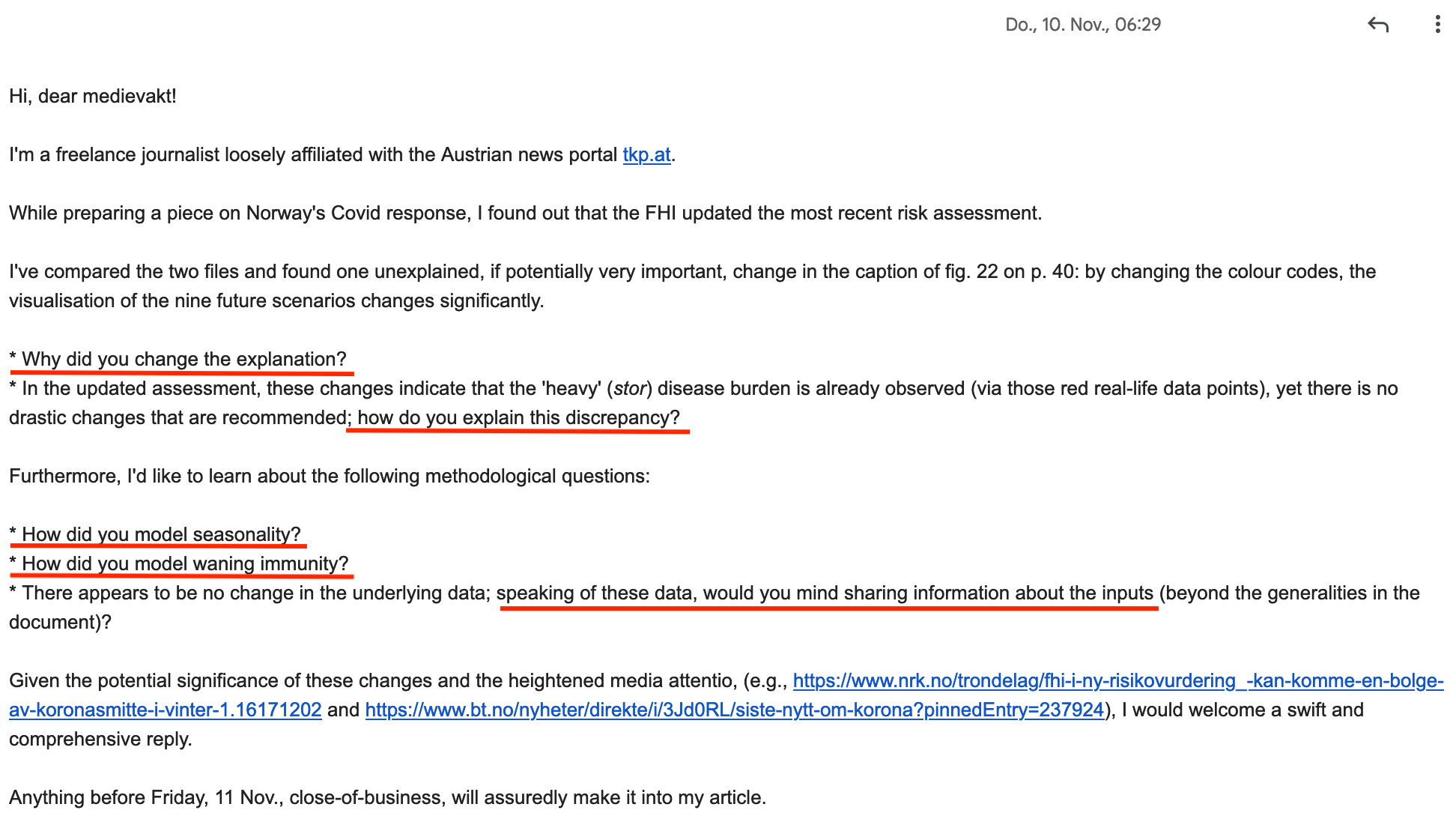
As is known to readers of these pages, on 8 Nov. 2022 the IPH came out with a new risk assessment. By pure chance I talked about it in a video meeting on 9 Nov.—and when I put together my posting on the day thereafter, I noticed one possibly significant change: without mention or explanation, the caption of the modelled scenarios about possible futures concerning Covid in Norway in winter 2022/23 had been changed. For particular, please see here:

As it happened, I sent an email to the IPH’s media department (I’m unsure it’s more than one person; every time I email them, it’s the same individual who signs the replies):
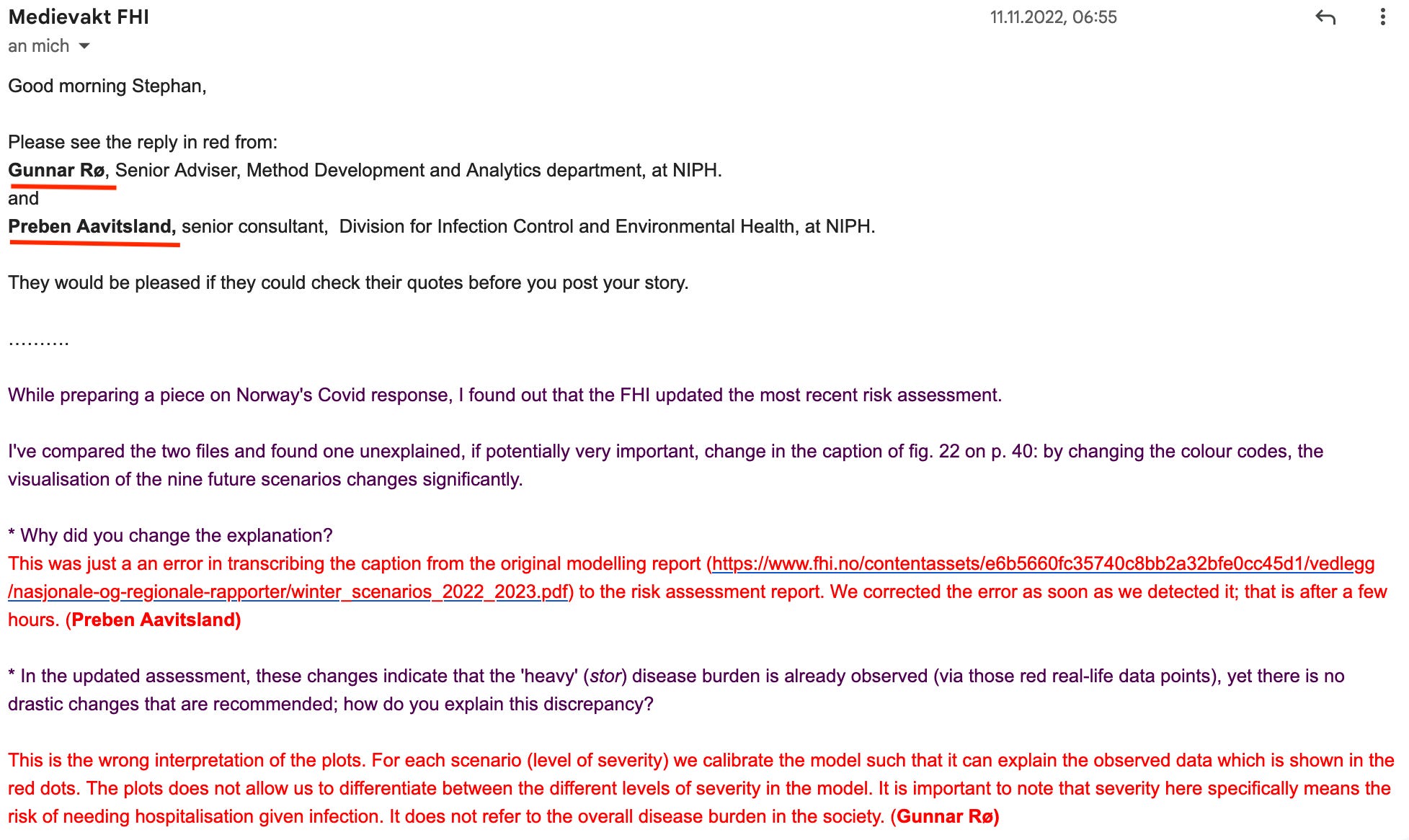
Imagine my surprise when, only a day later, I actually received a quite substantial answer, which I’ll also reproduce in full below (due to the length of the email, it’s split in two parts):
Now you know how I got my hands on the IPH’s data.
If there are statisticians and/or mathematicians among my readers (here’s looking at you, Joel Smalley and cm27874), what do you make of the modelling assumptions concerning seasonality?
Step 2: approaching Norman Fenton and Joel Smalley
Once I checked out the data, I contacted Norman and Joel to see if they would be interested in it. Sure enough, both replied quickly, we exchanged a few messages—and you all know what Joel did:

With Joel’s analysis in hand, I wrote another message to the IPH asking them the following questions:

Tell you the truth, I didn’t expect anything to come of it.
In the meantime, I went about writing my article.
Interlude: the part that’s not on my Substack (yet)
So, I did check out the parts I was pointed to by the IPH, specifically the documentation about the changed models, which you can find here. I specifically looked at the last three of this 17-page document, which is introduced with the header ‘immunity and waning’ (the document itself isn’t even paginated…), which provides the following explanations about the model (all emphases mine):
One of the major uncertainties related to the risk posed by Covid-19 in the present situation, is the overall level of immunity in the population. While we know exactly how many people have been vaccinated with each dose and at what time, we do not know how many have undergone infection. There is clear evidence that infection provides immunity against reinfection and severe disease, although the protection against reinfection wanes with time. In particular, the combination of vaccine and infection, so-called hybrid immunity, seems to give very strong protection, especially against severe disease. [note that no references are provided to back up these claims with, say, data]
Here are their assumptions that were fed into the model:
We assume that only doses 3 and 4 give any significant protection against Omicron infection [keep this in mind]
Figures A3 and A4 show…data on the distribution of previous infections by age, and the cumulative share of the population that has had an immunologically boosting event (vaccine or infection) as function of time, respectively. [oh, here infection counts again? I’m confused, which is it?]
How fast the protection against infection, from either vaccination or previous infection, wanes with time. We assume that protection wanes according to an exponential decay function. [ah, something I can understand; ‘protection’ deriving from 3 or 4 doses, or infection, wanes like Hemingway described people getting bankrupt: slowly, and then all of a sudden]
Thus fortified, we may now look at these models; do keep in mind that B.C. (before Covid), regulators typically didn’t green-light pharmaceutical products if their efficacy was below 50%, mainly because any effects may not be accurately determined to be due to the agent or to chance.
Oh, lest I forget, on the same page we also read the following:
We do not take into account any complications such as the fact that unvaccinated people are more likely to have been infected.
Now we’re quite ready to look at those wonderful models, which fall mainly in the category garbage in—garbage out: it’s only 3 or 4-dose recipients with or without infection, which may or may not count while there’s no control group (the ‘unvaccinated’). Note further that no data whatsoever is provided in, say, footnotes or the like.
In case you still want to see the results, well, here you go:
Well, you asked for it. At least we sort of knew that there’s a 7-day ‘grace period’ after the third injection, which means that the 50% threshold for pharmaceutical products would be ‘breached’ after 40 days in the ‘medium waning’ scenario and 27 days in the ‘fast waning’ scenario.
In other words: any protection doses three or four would afford its recipients would be basically indistinguishable from a chance event after 33 or 20 days beyond the last ‘immunological event’ (which, let’s keep this in mind, would be either an injection or an infection, or whatever, I suppose). Remember: no control group exists and it’s not even clear how these relative risk ratios were calculated given that the denominator (no. of infected individuals across Norway) is unknown.
Now we know. My tax money hard at-work.
Let’s move on before I will solicit a refund from the Tax Administration.
Step 3: Preben Aavitsland responds again—today
Now for the grand finale—I didn’t expect anyone from the IPH to actually respond; so, you may imagine how big my surprise was when I received another email by none other than Preben Aavitsland.
To me, my enquiries to get in touch with Preben (we’re in Norway, hence we’re all on a first-name basis anyways) always seemed Quixotic, of sorts, albeit in the none-too-good Roger and Me version of me, the spare-time freelance journalist (of sorts) trying to get answers from the chief epidemiologist and media attention junkie who happens to work on the ‘pandemic’ issues for the IPH.
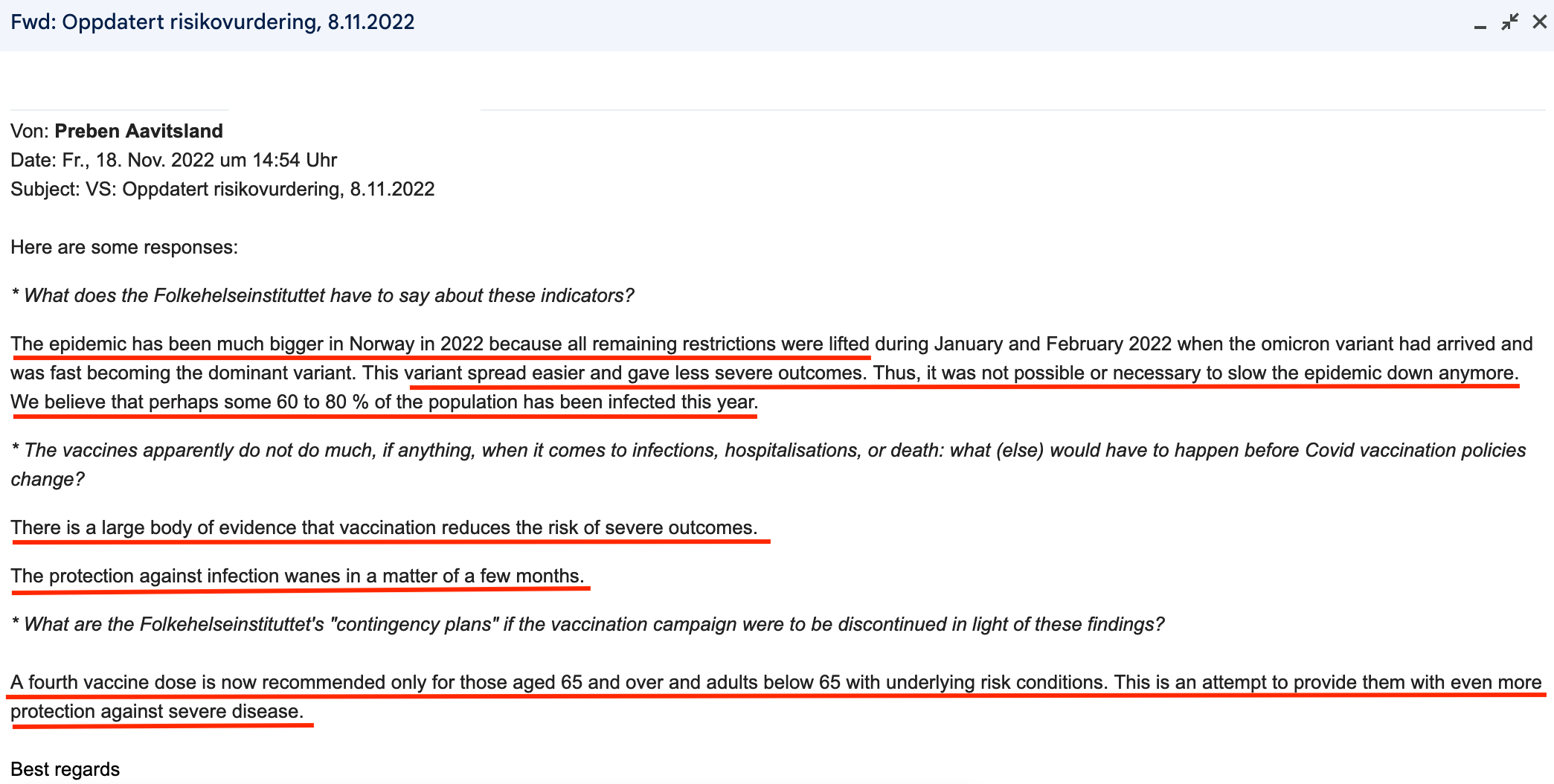
Here is Preben’s reply:
I hope you won’t consider it presumptuous of me to characterise these answers as either disingenuous, kind of not on topic, or otherwise not very helpful.
Sidenote to Joel Smalley: my friend, I think your data analysis is responsible for them even bothering to answer me, and I wish I’d had a ‘better’ answer from them at-all. Alas, one works with the answers one gets, not with the responses one wishes to receive.
My take on the IPH’s responses
Now these are statements, but hardly answers to my questions. As per Deputy Health Director Espen Nakstad, quoted in one of this week’s postings, indicates that almost 1.5m Norwegians have been proven to be infected (that is, PCR-positive). According to Aavitsland’s statement, however, the authorities reckon that between 3.25 and 4.3m people have probably been infected with Covid-19. What’s being off by 100-200% among public health officials?
Also exciting is the—in my opinion reversed—order in the first answer: Omicron was many times more contagious than earlier variants and causes less severe disease, hence it was possible to lift the measures. To me, it looks more like it was the other way round: due to Omicron’s higher transmissibility, the measures proved to be useless. At least the Norwegian authorities have come around to acknowledging this reality. Let’s not have Aavitsland or anyone else get away with this fake history (I’ve kept the receipts, by the way)
Aavitsland, on the other hand, failed to provide ‘answers’ to the question of the active substances (sic), but at least pointed to the rapidly declining effectiveness of the current preparations. If, however, the protection of the same decreases ‘within a few months’, calls or obligations to vaccinate are impossible for two reasons: on the one hand, as doing so means several injections per year (or disease season); given the speed of viral evolution under intense injection pressure, recourse would have to be made to untested active substances, on the other hand. We’ve also done that this autumn with the mice-steeled (/sarcasm) bivalent ‘boosters’; it doesn’t look like a winning argument.
At least, however, it does not seem, at the moment, that these facts are unknown; at any rate, I read Aavitsland’s last statement as recommending injections only for senior citizens and risk groups that way. However, I wonder how long these groups will be willing—or capable—to go along with this, if only because the risks associated with the repeated administration of modRNA products are hardly known, if they are communicated transparently at all.
Bottom Lines
First, the amalgamation of all three diagnostic codes (see here) led to the well-known progression and development of the ‘pandemic’, from the state of emergency to the discrimination of the ‘unvaccinated’ to health policy measures that seem more than questionable these days, especially in light of overcrowded emergency rooms, GP practices and hospitals (for example here or here).
Second, it should not be overlooked that the very amalgamation of all three diagnostic codes leads to the fact that, apart from methodological reservations concerning the data and in light of the high number of Covid-associated deaths since the Omicron wave subsided at the end of March 2022, there remain many questions about both the meaningfulness of the continued injection campaign, as well as the personal and institutional responsibility of the ‘vaccinators’ and their willing executioners.
Speaking of personal and institutional responsibility, there is also the question that these diagnosis codes were quite likely prescribed (recommended) by the very same public health bureaucrats pushing these policies to this day. I do believe it highly likely that there were instructions from highly-ranked public health officials who told every MD in the country to more or less code everything that even looked like a respiratory disease with R991 (presumed/probable), thus creating the ‘data basis’ for the declaration of the ‘pandemic’ in the first place.
There is still a long way ahead of us before we get answers to these and many other questions.
The struggle for truth, personal and institutional responsibility, and the future of our society continues.
Omg, they must absolutely hate us. At least, I now know at least one of the 6 numpties who answered "it would have been worse but for the vaccines" in my poll! Next time you email him, please ask about my bridge. Is he interested??
Stephan,
Excuse my ignorance of Norway, but when Aavitsland says "there is a large body of evidence...", is he referring to independent research done in Norway on vaccine efficacy, or, is he relying on the evidence provided by Pfizer and Moderna which gets uncritically recycled by the American CDC (which we recently learned shares the same PR firm as Pfizer [1])?
Perhaps in your next email ask him if it's possible that the reason every single country that vaccinated it's population saw cases explode and excess mortality increase isn't because "omicron was more transmissible" but rather, the vaccine had the same known problem of all previous SARS vaccine attempts - it made the host more susceptible to variants like Omicron. It was the reason we didn't have a working SARS vaccine despite 15 years of trying in the first place. [2]
[1] https://disinformationchronicle.substack.com/p/weber-shandwick-provides-pr-for-moderna
[2] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7094954/