


Covid in Norway: IPH Admits VE is 53% vs. Omicron--for 20 days post dose 2, gone thereafter; IPH also Confirms Vaxx Shedding by Nursing Moms
IPH also admits, tacitly, that no long-term VE data exists (doh), but keeps on recommending injections while more than 90% of hospitalisations occur among 'booster' recipients: Clown World

Just when I was getting happy to take a break from all matters Covid in Norway, the Institute of Public Health (IPH) has published a revised, or updated, Risk Assessment.
This posting will therefore be about Norway, again, but fear not, after this one, I shall take a break and humour you with something else of equally disturbing character.
Like its most recent ancestor from late March, this report continues the ‘Flurona’ saga by conflating the epidemiological situations related to, and deriving from, both Covid-19 and Influenza. The following accounting consists of a dedicated ‘executive summary’, followed by in-depth commentary, replete with relevant quotes, from the rest of the assessment. As always, if not noted otherwise, all emphases are mine.
Executive Summary (pp. 5-6)
The Covid-19 epidemic continues to be impossible to forecast [er fortsatt uforutsigbar], hence close monitoring and increased preparedness to deal with any change…is necessary.
After this introductory statement, I first thought that no further comment is required: as I pointed out time and again, we’re not just ‘flying blind’, but we also keep asking these experts and institutions to provide us with guidance. They fail about as predictably to do so as the sun rises in the east every morning. In other words: ass-covering, Norwegian style.
Still, the ‘winter wave is fast receding’, and this is borne out by all indicators, esp. hospitalisations (545 in week 9, now 137 in week 16, but the IPH somehow forgot to mention that the ratio between ‘un/vaxxed’ is 1 : 10, i.e., there’s now 10X as many ‘vaccinated’ than ‘unvaccinated admissions). Most Norwegians came down with BA.2, and also the Influenza A (H3N2) epidemic is receding by now.
In terms of risk, the IPH holds that Covid-19 will retreat even further during May, but this decline will be slower than in April. The money wording is this:
It is uncertain how small the epidemic’s [effect] will be and how long it will remain so; population immunity [befolkningsimmunitet] and seasonal effects also affect this…
A completely new variant can change this picture significantly, but the population’s basic immunity [grunnimmunitet] will probably protect well against serious illness, regardless of variant. Nevertheless, enhanced preparedness and monitoring is required.
Because these experts were so right about these things in the past, keep in mind that blindly following their guidance is of utmost importance. I’ve highlighted the two more essential aspects here, and I shall ask you to keep these in mind: current levels of immunity ‘will probably protect…regardless of variant’, which requires ‘enhanced preparedness and monitoring’—if you didn’t like the intrusive mandates and measures of the past two years, you’ll probably don’t like their continuation.
In terms of handling, surveillance, and preparedness, the IPH continues to uphold its conclusions from late March:
Society may continue with normal everyday life without significant anti-Covid measures…the population must be prepared for a stronger return of the epidemic and should be prepared appropriately.
Bits and Pieces about Covid-19
In this part, I shall highlight a couple of things I found quite interesting in terms of admission by Western public health authority (sic), so let’s jump right in, shall we?
Admission with vs. for Covid-19
First up, some historical data in Fig. 1 (p. 7), which shows that ‘hospitalisations for Covid as main cause, incl. ICU admission, rose significantly [betydelig] during the Omicron wave’.

Ha, you won’t believe it: there’s even one datapoint on ‘incidental’ Covid-19 positivity (p. 8). For the first time since 22 March, we learn that ‘on 27 April, there were 300 patients with Covid-19, of whom 163 had Covid-19 as main cause of admission’. This is interesting in its own right, for last time the IPH shared these data with the public, the ratio between admission with vs. for Covid-19 was 13 : 1. Now it’s back in the 2 : 1 range, probably in line with the receding Omicron wave. Still, what I found quite troubling is the ICU admission number: of these 163 patients hospitalized for Covid-19, 37 (or c. 23%) ended up in the ICU.
Influenza in Norway: A Dual Outlier
Likewise, Fig. 3 (p. 8) is curious: this season (black line), influenza came around very late, and the same records also show how much of an outlier its non-existence in 2020/21 really was:

To me, this makes me wonder about just what could have occurred in 2020/21 that caused ‘influenza-like illness’ and case fatalities. In addition, why do we count influenza waves in seasons that change year-on-year while we don’t do so with Covid-19? Being no expert in these matters, all I can do is wonder…
Covid Elsewhere (pp. 14-19)
I’ll skip over the influenza bits and pieces in-between, and most of the Covid Elsewhere items as well, for there’s not much of interest there (IPH uses official data compiled by OWID, hence something you and I can do as well); if you’re data-driven, it’s worth a look as they also footnote and link to the most recent official statements and some pre-print studies.
I shall only share two images from these pages, which I find particularly telling. These are juxtapositions of Fig. 11 (OWID-deriving data on ‘cases’, hospitalisations, ICU admissions, and deaths in France, Germany, the Netherlands, and the UK, p. 16), which the IPH compares to—South Africa, a well-known public health powerhouse:
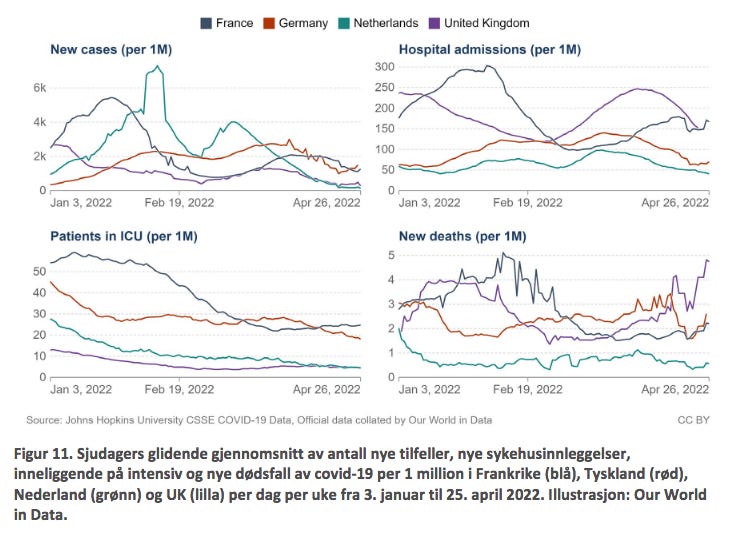
See if you can spot the difference (p. 17):

If, at this point, you keep wondering just how Israel, Pfizer’s real-world lab rats, are doing, well, the IPH remains silent on this one (but you can go to OWID and find out; I won’t reproduce these data here, but it’s an ‘uncomfortable’ comparison…)
With these curiosities highlighted, let’s now turn to some of the more interesting pieces of the assessment.
Some News from the IPH (pp. 20-21)
There’s the following paragraphs on ‘vaccine efficacy in the young’ (12-17yo) from August 2021 to January 2022; there’s a recent IPH-sponsored pre-print that covers both Delta and Omicron with respect to the BioNTech/Pfizer product (Comirnaty), which I shall reproduce in full:
After two doses, there was over 93% protection against the Delta variant for the first eight weeks and then 84% protection. The corresponding protection against Omicron was 53% [for the first eight weeks] and then 23%. The researchers conclude that vaccine protection against Omicron is poorer and deteriorates faster compared to Delta.
The IPH’s statement derives from this pre-print by Veneti et al., entitled ‘Vaccine effectiveness with BNT162b2 (Comirnaty, Pfizer-BioNTech) vaccine against reported SARS-CoV-2 Delta and Omicron infection among adolescents, Norway, August 2021 to January 2022’. You may find the paper here.
Published as a pre-print on 25 March 2022, this is quite something in terms of recent data that also allows for comparisons of both Delta vs. Omicron. It’s a population-based cohort study employing Cox proportional hazard models to estimate vaccine effectiveness (VE). To me as a non-epidemiologist, the following methodological considerations suggest it’s an actually quite well-done study (please, if you know better, let me know):
Vaccine status was included as a time-varying covariate and models were adjusted for age, sex, comorbidities, county of residence, country of birth, and living conditions. Data were obtained from the National Preparedness registry for COVID-19, which contains individual-level data from national health and administrative registries.
So, how do Veneti el al.’s findings compare with what the IPH published? You be the judge:

To me, this looks suspiciously like lying by omission (even though at this point, I’d call this intentional). Still, look at the findings of VE against Omicron: ‘no protection against Omicron after receiving one dose’, yet the IPH still recommends that
children and adolescents born between 2006-2009 can [kan, emphasis in the original] receive both doses 1 and 2 if they of their parents ask for it
Dose 1 will reduce the already low risk of a severe course of Covid-19 [my emphasis]
Dose 2 can also have positive use [nytte], but its effects are limited since the risk of a severe course of disease is very low after the first injection
You can clearly see how the IPH spins this, even though their own data must be very painful to acknowledge for whoever wrote this, as well as for anyone of these spineless critters who approved this piece of junk.
Vaccine Protection lasts…20 Days
Basically, the IPH is telling everyone who cares to dig through this assessment that no-one under age 18 should get this piece of crap. Look, again, at VE among 16-17yo: it ‘peaked at 53%…in 7-34 days after the second dose’, according to Veneti et al.
Translation: subtract the by now-customary 14 days from the higher number (34 days) and 16-17yo get a maximum protection of 53% for less than three weeks. Beyond that, VE ‘decreased to 23%…in 62 days or more after vaccination’.
These are coin-flip-like odds to begin with that, with VE ‘decreas[ing] with time since vaccination for both variants, but waning was observed to occur faster for Omicron’.
At this point, I’m left wondering as to why they don’t publish such data for adults (even though I fear I ‘know’ what that data would say…)

Hear, hear!
There’s also mention of another pre-print (Whittaker et al.) that assessed risk of severe Covid-19 and MIS-C (multi-system inflammatory system in children) across the Alpha, Delta, and Omicron waves by analysing data from Norway. Its main findings include…
Risk reduction from Alpha through Delta to Omicron
Children and adolescents have very low risks of severe Covid-19
Remember, all study participants were both unvaccinated and Covid-naïve
Vaccine Shedding
Still, there is this paragraph that relates to…shedding (which remains, of course, unmentioned explicitly here):

Also, do make the effort to scroll down to Table 1 on p. 21 in this pre-print.
In a sane world, these findings, however preliminary they may be, would be front-page news. They are indicative of large-scale fraud by Big Pharma and the corruption of both public health authorities and government.
In a sane world, this is a done case for any state attorney.
If you check Norwegian media, though, well…crickets (e.g., here or here)
Immunity Against Sars-Cov-2 (pp. 25-26)
This is a kind of ‘best of’ the IPH’s tacit, if quite outspoken (comparatively speaking) about-face, at least to me:
Immunity can come from vaccination, infection, and the combination of these (hybrid immunity).
Note that there’s no more ambiguity about the de facto admission of equivalence between these categories. It’s not just that natural immunity is back in business, but its implication—logically, there must not be any differentiation between the validity of, say, one’s ‘vaccination status’ (currently 360 days if you’ve taken a booster) and ‘recovery’ (180 days, both via the EU’s guidelines).
There’s more:
Neutralizing antibodies protect against the establishment of the infection in the body, while cellular immune responses (T cells) mainly protect against serious illness and death after an infection has been established. This means that even if antibody levels are gradually reduced to below a level that protects against infection, the protection against serious illness and death will remain present as long as cellular responses are maintained, and the immune system is ready to mobilize antibodies (from memory B cells) quickly and powerfully. The time course of the deterioration of immunity and reduced protection after vaccination may be affected by conditions such as age, immune status and general state of health.
So, the way I read as a non-expert read this is the following: we’re setting you up for the significant decline of the injection-induced high levels of antibodies (which we only know about for a few weeks post-injection anyways). Talk about normalisation of not just the obvious, but as long as we don’t ‘measure’ anything related to cellular immune response, there’s really no more point in checking anyone’s injection status (not that there ever was any rational reason to begin with…)
We thus expect protection to decline somewhat over time. It is not well enough known how the number of vaccine doses and the number of infections with different virus variants, as well as the time intervals between events, affect the preservation of immunity.
Protection against infection and transmission deteriorates faster than protection against serious illness. This can largely be explained by the fact that neutralising antibodies naturally decrease faster, while the cellular immune system persists considerably longer.
See the sleight of hand? Every public health authority has denied these essentials of ‘Immunology 101’ for the past 1.5 years. While I personally see this as a major change, given that no-one appears to care what Norway does—esp. compared to, say, Sweden or Denmark—this is but an admission of both failure and the IPH’s ignorance.
And it is awful, for a few pages earlier, the IPH’s own researchers have documented in no uncertain term (see the Veneti et al. paper above) that VE is de facto a coin flip for about three weeks post dose 2 and about all but gone two months later.
Furthermore, and public health authority that retains its recommendations to ‘get vaccinated’ any longer is engaged in serious fraud, conspiracy, negligence, and malfeasance. Note that these are all criminal acts.
Vaccine protection against serious illness in the general population is high shortly after vaccination with the first booster dose. We have little knowledge about the duration of this protection due to the short follow-up time. The protection decreases minimally in the first 2-3 months after vaccination, also among the elderly over the age of 65. A combination of vaccination and SARS-CoV-2 infection provides high protection against serious illness in the general population. There are so far no definite signs of impaired protection against serious illness among people with vaccination with three doses, regardless of age.
I’ll interrupt the flow here for a second or two: there’s more admissions of ignorance, but how can these people over at the IPH write this—after pointing to the two papers cited above?
Furthermore, here’s the key data plot from the IPH’s own most recent report (week 17, see here for the source, with Fig. 6 on p. 11):

Please look at Fig. 6 and tell me that there’s ‘no definite signs of impaired protection against serious illness among people with vaccination with three doses’, and while you’re at it, do consider the following chart showing injection uptake across all age brackets (ibid., p. 55)

And now you get to look at the age distribution of hospital admission again (ibid., p. 10):

No signals, eh?
Comments and Conclusions
I’ll wrap this up with the following two paragraphs from the risk assessment (p. 26) that functions as pathetic attempts of ass-covering here:
A small weakening of protection can be of great significance. For example, a reduction in the proportion protected against serious illness from 90% to 80% would mean a doubling of the number of serious cases, given an equally large epidemic.
A new variant can change this image. It is nevertheless likely that the protection against serious illness will be well preserved also against new variants.
You see, VE dropped considerably against Delta (to 84%, down from 93%), according to Veneti et al. It was even worse against Omicron, yet however they do it, IPH maintains that ‘it is nevertheless likely that the protection against serious illness will be well preserved also against new variants’.
I call BS on this one, and my only explanation is that there’s professionals and experts drafting these reports—and then there’s the political appointees and spineless critters who alter them according to the way the winds are blowing.
This is about as much as you can take away from this assessment, other than: if you haven’t taken these products, don’t start. If they ‘worked’ so badly so far, you don’t want to imagine how much worse they may ‘perform’ in the future.
I’ll leave you with the IPH’s assessment for May 2022 (pp. 30-31), and invite you to draw your own conclusions and share them with me and the other readers in the comments below:
The winter wave is over…It is uncertain how the epidemic will develop…[as] population immunity and seasonal effects affect this.
The number of new admissions for Covid-19 will probably continue to decline through May, but not as fast as in April, and the decline in the admission curve may flatten out during May.
The consequences of the epidemic in May for society are decreasing further…For individuals, the consequence is that fewer and fewer will become infected.
We must expect a new wave with the [Omicron BA.2] variant, likely in the autumn or next winter, or a new wave of a new variant already this summer.
The situation is thus still unpredictable. A completely new variant can change the picture significantly, but the population’s basic immunity [grunnimmunitet] will probably protect well against serious illness, regardless of variant. Nevertheless, enhanced preparedness and monitoring is needed.
There you have it—there will be more of the same, or of something worse, and while the IPH spent half the assessment telling everyone who cares to read the fine print that ‘the vaccines’ have failed against Omicron, what they’re not telling you is—that they’re betting everything on injections plus infections.
Oh, and they want to increase surveillance, you know, just in case.
Covid in Norway in one Chart
Lest you wish to assess the numbers for yourself, here’s Tab. 1 from the assessment (p. 27):

It shows the current status of Covid in Norway, which means…
89% of all deaths occurred in people 70 and older
87% of all ICU admissions occurred in people 40 and older (albeit that share, too, is heavily biased towards seniors and those with comorbidities)
82% of all hospitalisations for Covid-19 occurred in people 40 and older (same caveats apply)
And keep in mind that people 60 and older represent only 5.7% of all those Norwegians who test positive for Sars-Cov-2
Please share this widely, maybe, just maybe, Norwegian data might have an impact.
Epitmetheus, bombshell in Italy! Yesterday Prof.Bizzarri, during an audition organized by some Senators, dropped all the heavy bombs on the fake narrative, lies and frauds. Asking the Health Minister "Speranza" to act against those. He's a patholigist, oncologist, researcher and head of Pathology world Association. Here the main part of it on the Tube:
https://www.youtube.com/watch?v=bcqDDq16VEQ
Here the Sen.Paragone one of the main organizer of the audition:
https://www.ilparagone.it/attualita/sul-covid-montagnier-aveva-ragione-anche-se-gli-davano-del-pazzo-la-spiegazione-delloncologo-bizzarri/
There's a term for progressively lower efficacy of the injections against each successive variant. Evolutionary escape. The papers cited above seem to tacitly admit that these new variants are evolving to evade injected "immunity," which could only have happened with their policy of mass-injection, even of the recovered, during the plandemic with a defective "vaccine." Note there is no corresponding deterioration of natural immunity suggested. They did this to us.