
Covid in Norway: Data for Week 16 shows Differential b/w Un/Vaxxed Admissions to be 1:10--the 'Pandemic' is All But Over for 'the Unvaxxed'
Also, AE incidence per injection for kids 5-11 is 1:441-574--wtf are we doing?

Guess what—the latest weekly update has been published by the Institute of Public Health (IPH), which provides the following ‘insights’ into…well, since there’s no more comparison with ‘incidental’ admissions with Covid for a month now (see here for a summary) this will have to do. As a ‘bonus feature’, I’ll throw in some considerations about AE incidence in children aged 5-11.
Key Data Points from Week 16
The first post-Easter weekly update was trotted out without fanfare—and I shall provide a very brief account of the update for week 16 (18-24 April 2022).
Even though the Omicron (BA.2) wave is receding, it doesn’t do so as fast as hoped for, modelled, or expected (or a combination thereof). Admission numbers were adjusted upwards significantly for last week (in my original post, the IPH spoke of 131, now we learn it were really 152). Mind you, Norway only counts admissions for Covid-19 as main cause, hence, at least these numbers are o.k.-ish in terms of reliability.
Odds for admission continue to be quite elevated among senior citizens, in particular among those 75 years and older.
As regards Covid-associated deaths, the tally now stands at 2,932 (up from 2,871 in the previous report), with the peak of these deaths occurring in week 11. By now, about 2/3 of all Covid-associated deaths ‘occur in hospitals and care homes’ (p. 3).
Speaking of dying, the IPH now admits (ibid.) to excess mortality beyond the otherwise expectable range ‘in weeks 8, 9, 11, 12, and 14’, in particular affecting ‘those age groups 65 and older’, which showed excess mortality ‘in weeks 8-12 and 14’. (Looks like it’s Omicron that killed grandpa and granny, as opposed to the unclean unvaxxed…)
Testing data continues to crapify, with the report actually reading:
Data from the polling tool Symptometer shows that after week 8 there was an unknown reduction in the share of participants who reported symptoms of the common cold, the share who self-registered [Sars-Cov-2] self-testing, and the share of those who tested positive.
Apparently, irony, self-respect, or even proof-reading their own statements never occurred once to the good people over at the IPH who compose these reports. It’s a wonderful way of telling the world (ahem) that whatever testing data is coming out with respect to Omicron is, well, horse manure-grade quality (with due apologies to all horses). I only included it to highlight this nugget, which might also encourage you, my dear readers, to look for comparable ‘admissions’ in other countries. If testing data was problematic to begin with (ahem), it’s now admitted being absolutely meaningless, with its continued usefulness (?) for virtue-signalling purposes perhaps being the only purpose left.
Sidenote: Symptometer is an IPH-run tool that allows select GPs, family doctors, and local ERs (legevakt) to add patient data anonymously into a database that, as far as I understand it, is supposedly representative of Norway, which in turn allows public health authorities to estimate the overall pressure on healthcare providers. As such, it appears helpful, if not useful, at first, but to me only until you actually read that what they do is actually compile yet another database based on an even larger number of other databases than those the IPH is already struggling to analyse in the first place. Talk about ‘complexity’…
Injection uptake continues to flatline. The numbers haven’t changed since late March, and the share of the total population who received two doses remains at 73% (88% of 16+ and 89% of 18+); 83% of 16-17yo and 55% of 12-15yo received one injection; 43% of 16-17yo received two injections. These numbers are essentially the same as of 27 March, with the minimal increase of 1% update in the 12-15yo bracket being the only change.
Same with ‘boosters’—no changes: 53% of the entire population received a third injection; the share is 90% among 65+, 82% for 45+, and 66% for 18+. Among vulnerable groups, 81% of all 18-64yo in high-risk groups received a ‘booster’, as opposed to 74% (here there’s also a 1% increase) in moderate risk groups.
Omicron BA.2 surpassed BA.1 in week 6 (mid-February) and now constitutes around 98% of all sequenced tissue samples from the past two weeks. No significant changes to the virus were observed in the past two weeks, with perhaps the exception of ‘sporadic’ (p. 3) occurrences of the BA.5 variant, about which I’ll write a bit more down below.
Assessment by the IPH (p. 4, my emphases)
High vaccination coverage contributes to protection against severe Covid-19. The Omicron variant has also lower inherent virulence. The risk of serious illness is therefore very low for most infected people. Severe Covid-19 now particularly affects unvaccinated people and vaccinated people with old age or underlying diseases. It is still important that unvaccinated people start their vaccination, and that people over the age of 45 and medical risk groups over the age of 18 take a booster dose.
I’ve highlighted a few parts that we shall take a look at in the following. Before we do so, there’s more to the report than meets the eye, specifically this:
The Covid-19 pandemic is still ongoing. Although the epidemic in Norway is currently receding quickly, there is a need for strengthened surveillance, good plans and increased preparedness to meet any changes in the situation. There is still a risk of new waves of Covid-19 with Omicron-like variants or with completely new and more virulent variants that may also escape today’s vaccines.
In other words: the IPH copy’n’pasted their ‘assessment’ from last week’s report. Let’s look at how the numbers have changed, though, for there has been quite a bit of change.
Hospitalisation and Death Numbers for ‘Unvaxxed’ Plummet, Rise for ‘Boosted’
Only a few words are necessary to convey the current state, so here goes.
First up, Tab. 3 (p. 7), which shows the spatial distribution, with ‘South-East’ (Sør-Øst) firmly leading the pack. In other words, this was, as I mentioned months ago, quite an Oslo metro area phenomenon, whose admissions exceed the rest of the country’s by a magnitude.

Next up, age distribution by visualisation and numbers (Fig. 3, p. 9, and Tab. 4, p. 10, respectively). While I think these are quite self-explanatory, I’ve added a couple of question marks to the one age bracket whose admission incidence is currently on the rise (74-84). While I don’t know why, I dare to guess: among the oldest cohorts (85+), hospitalised individuals may be too frail to get ‘the shot’, or they remain in care homes. I suspect that the flip side of this coin would be: those 75-84yo who end up in the hospital because of Covid-19 may be those who are jabbed, but it’s a guess…

As always, the most informative table comes with the no. 6 (p. 11), which shows everyone who cares to see—which incl. very much Andreas Oehler’s recent post on Ontario, Canada that shows virtually identical ratios—of admissions of ‘unclean’ vs. ‘all-cause injected’:

Yep, you saw that correctly: for every ‘unvaccinated’ admission for Covid-19 as main cause, there’s ten individuals who received two or more injections. That’s an order of magnitude. Let that sink in for a moment or two.
So, how big a fvcking deal is this difference? Well, here goes…
The overall share of Norway’s residential population who received any number of doses stands at 73%. In other words: while there’s only some 27% ‘unvaccinated’ remaining, as per Tab. 24 (p. 55, below, with references omitted), they represent only 1/10 of the admissions for Covid-19 during the past four weeks.
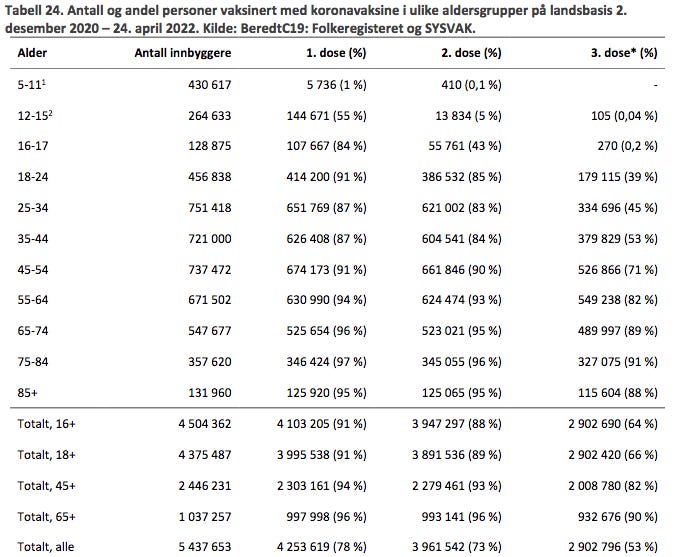
Note the almost complete synchronicity in injection uptake from age 45 upwards: the differences between doses 1 and 2 is typically around 1%; ‘booster’ uptake is a bit more variegated, so to speak, but it’s still insanely high among those 45 and older (which might be Norway’s way to ‘solve’ the retirement funding problem…)
By the way, if you compared week 16’s Tab. 6 (see above) with the same Tab. 6 from as recent as the report from week 15 (yep, a week earlier), you clearly see what has changed and by how much:
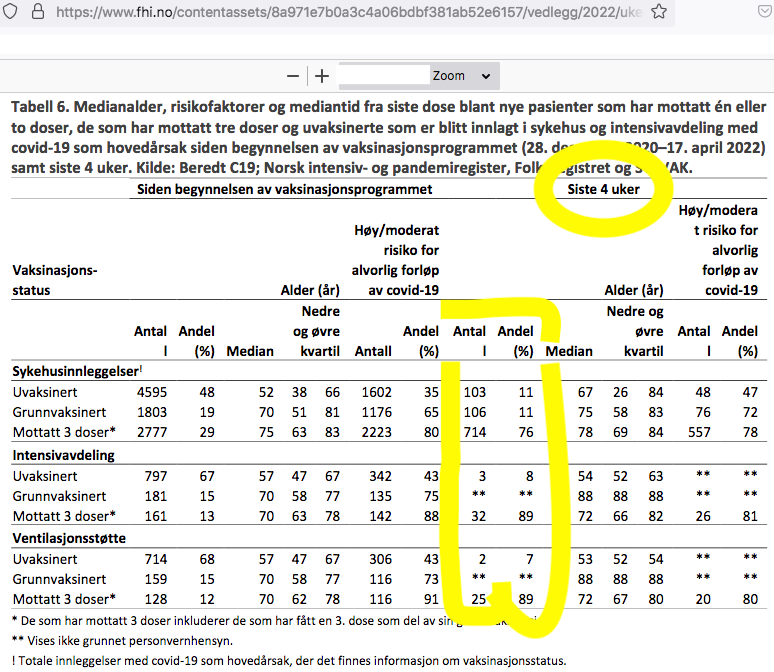
Note again the highlighted ‘last four weeks’ (siste 4 uker) section: ‘hospitalisations’ (skyehusinleggelser) among ‘unvaccinated’ stood at 103 vs. 820 for ‘any number of doses’. In week 16, the same category merely shows 67 vs. 664—an almost percent 1:10 ratio, which compares ever more favourably to the 1:8 ratio of a week ago. If you wish to, you may also check out earlier iterations of Tab. 6 (by simply going to my posting archive and look for Covid in Norway; spoiler alert: that ratio was 1:2 as recent as week 7 and 1.4:1 in week 52).
In other words: Omicron has spoiled the vaccinators’ game. I think that the evidence is conclusive.
To round off this section, here’s the customary visualisation, Fig. 4 (p. 12):

Last Words: Covid-associated Deaths
Speaking of ‘conclusions’—of life, in particular—below Table 8 is on p. 16. Again, note the last four weeks, which show that a mere 11% of all Covid-associated deaths occurred among ‘the unvaccinated’ (that share was 14% in last week’s report), which is a slightly better death ratio of 1:9 (that ratio was 1:7 in last week’s report) and compares favourably to…your odds of hospitalisation, if you took any number of these injections.

Bonus Feature: AE Incidence Among 5-11yo
While compiling the above information, I noticed something odd, and it related specifically to that incidental inclusion of Tab. 24 (showing injection uptake) broken down among age cohorts.
Tab. 24 (p. 55) holds that of 430,617 residents in that age bracket 5-11, 5,736 (or 1%) have received one dose, with 410 of these (or 0.1%) having received also a second dose. No booster injections have yet been administered to children in this age bracket.
If you have eagle eyes, you may have noted a footnote (1) in the above Tab. 24, which informs the reader that, among this particular age group, ‘only those belonging to select risk groups were eligible until 14 Jan. 2022, and that the vaccine will be available to all from the end of January onwards’.
Now, as mentioned by el gato malo in yesterday’s post, Denmark declared it would ‘suspend’ its mass vaccination campaign in mid-May. This is kinda important (not only because the Nordic countries closely eye and follow each other), for there’s virtually no increase in injection uptake in the 5-11yo bracket (thank God) since it became available to all 430,617 children.
Why, we may now ask, right?
Well, to me, it would appear quite easily explainable by taking another look at the AE reporting done by the National Medicines Agency (Legemiddelsverket) whose latest report (dated 19 April 2022) provides the following information:

You see, there were ‘<20’ suspected AEs, which, in the context of the above uptake of 5,736 (dose 1) means that the AE incidence is insanely high: there were 9 ‘AEs of light severity’ (lite alvorlige meldinger) plus ‘<5’ ‘severe AEs’ (alvorlige meldinger), which allows us to calculate, however crudely, the AE incidence for children aged 5-11:
The AE incidence ranges somewhere between 1 AE for every 441 injections (basis: 9 ‘light’ AEs plus 4 ‘severe’ AEs) and 1 AE for every 574 injections (9 ‘light’ AEs plus 1 ‘severe’ AE).
If you thought that this is an insanely high ratio, wait until you read the below section (p. 8), which I’ve translated in full (emphases mine):

On 14 January 2022, the vaccination offer was expanded to include children between the ages of 5 and 11. At the same time, children aged 12-15 became eligible to receive two doses. Case processing of suspected AE reports in children and adolescents are a high priority. We follow closely and are especially attentive, if serious incidents are reported after vaccination.
Adolescents most often experience the same common and transient side effects as adults after vaccination.
As of 19 April, more than 467,000 doses have been administered to children and young people aged 12 to 17. In the period from December 2020 to 19 April 2022, we have processed 592 adverse reaction reports in the age group 12-17 years. Of these, 78 are classified as serious. This includes seven reports of heart inflammation, pericarditis and myocarditis [see here for my previous work on Norwegian AE tracking]. 80% of the side effects reports in this age group are from girls. Many reports concern menstrual disorders. Most are classified as not very serious. [Is this presumably mainly middle-aged men talking about menstrual disturbances among teenage girls?]
So far, more than 5,660 children in the age group 5 to 11 have been vaccinated. We have received and processed less than 20 reports of suspected side effects in this age group.
Check out that last paragraph again: ‘less than 20 reports of suspected side effects’ sounds a lot ‘better’ than 1 child in every 441-574 injections experiences any kind of AE.
Final words for now: we can easily observe the state of any society by checking out how ‘they’ treat the least among them, in particular children. Apparently, the injection numbers in this particular age cohort haven’t (thank God) moved upwards.
WTF are we doing to our children, to ourselves?
One great problem with debating the issue of covid, how dangerous it actually is, and the mRNA-shots (aside from what can only be called "superliminal" propaganda and censorship and so on) is the sad fact that media - at least in Sweden - has continously picked out the most deranged critics as being typical of all critics.
It's an old-school propaganda tool of course, very effective here in the nation where the socialist democrats tried to make it illegal to own satellite-dishes for private citizens or to receive foreign radio and TV (especially news) in the late eighties: for at least 75% of swedish swedes, if it's not on state TV or radio, or in any of the old regime loyal legacy papers, it's not real and must be disinformation.
However, there is also the sad fact that a great many public critics are of the "chlorine is used to bleach sugar"-variety. Incoherent, raving, neurotic, paranoid, and equally myopic as any politruk or apparatchik or corporate creature - just in the opposite direction: if it's /not/ from a pharmaceutical company, and not checked out by regulatory authorites, and (even better) is "natural" and (best of all) african or asian, it is guaranteed to be a good cure for any ailment.
Which is of course is as patently ridiculous as the claims of various corporate and political critters these past two years. You could say that just because being shot in the left foot is bad, does not make shooting oneself in the right one good.
We are following along with the century old indoctrination. Also, the government purchased the injection and that contract the government signed with the manufacturer ought to be investigated. You know what I think already we have to go back.