


Covid in Norway—Christmas Edition: no-one knows much, and no-one wants to be in charge
The IPH came out with a new fear-ridden 'assessment' on 22 Dec. 2021, which shows that they read 1-2 week-old data to say 'we don't know'

So, less than 10 days after the Norwegian Institute of Public Health (IPH) recommended stronger measures due to fear of Omicron, an updated version of their risk assessment was published.
This comes at the heels of a hectic week in Norway: while ‘cases’ are receding (with everyone in charge claiming that’s the effect of the booster jabs), the government is contemplating its next steps. Legacy media is slowly catching on that some of the wildest claims of both the IPH and the Norwegian gov’t were, in fact, claims, as, e.g., a short piece in Aftenposten (paywalled) from last weekend suggests.
Curiously enough, earlier this week, the very same journalists of Aftenposten (Per Anders Johansen and Ole Alexander Saue) came out with a report that documented waning support among Norwegians for the new restrictions: less than half of the population, it is alleged, was with the government on this. Why, you may ask? It’s mainly because no-one over at the IPH may actually say something substantial about the success (or lack thereof) of these restrictions and that, according to Bergens Tidende earlier on 22 Dec., is ‘quite embarrassing’.
Also, there were more press briefings and more things to be said about all of this, and the main points of the IPH’s updated assessment are:
Omicron will bring a new wave in January due to the variant’s greater transmissibility, yet it is uncertain how big that wave will be. This depends on [Omicron], its spread, the effect of vaccination, and the effects of infection control measures as well as behavioural adjustments.
There is large uncertainty about future developments. Vigilance, readiness in the health sector, and preparedness at the local level are necessary if new measures must be introduced.
So far, so much boilerplate. Yes, there’s a ‘flattening’ of the upward surge of ‘cases’ in the past couple of days, which appears to be mainly due to the rapid distribution of ‘booster jabs’, despite all internationally-voiced concerns (see here for WHO chief Ghebreyesus at a recent press conference and click here for Robert Malone’s take).
Basically, the IPH admits that they don’t know what’s going to happen with Omicron next.
Let’s have a look at what the IPH had to say in its ‘updated Covid-19 risk assessment (there’s of course more, but this will have to wait for another post):
About that updated risk assessment
As explained on pp. 6-7, there is certainly quite an increase in respiratory infections these days. Yet, it’s almost Christmas, hence, most of these issues are seasonal (i.e., to be expected). Do note, and the below images are on pp. 8, that what is odd this winter is that spring bulge of Covid-related hospitalisations in March, April, and May 2021 (Fig. 4), but do note that at the beginning of 2021, these numbers were around 100—which right now the range of 250-350 (see the left-hand side for ‘regular’ admissions, the right-hand side gives ICU admissions):

Fig. 5 (p. 8) shows the increase of hospitalisations in the final quarter of 2021; do pay particular attention to the beginning of the data set in week 39 (bottom left corner), for this will become important in a moment. Basically, whatever happened after mid-September 2021 happened to middle-aged and senior citizens (see the magenta and grey bars in the below figure).

Given the geographical distribution of Norway’s population, it’s hardly surprising that most of the action—pressure on healthcare providers—actually occurs in the country’s south-east, i.e., in the Oslo metro area. This can be clearly seen in the below illustrations 6 and 7 (p. 9), which show total hospital admissions (incl. ICU, fig. 6) and the regional breakdown (fig. 7).

Elective Affinities: Trends in Hospitalisations, weeks 47-50
As the report and virtually all legacy media will not tire these days, December was the month the trend turned: ‘about half of all admissions for Covid-19 as main cause, even though that group constitutes only 10% of the population [eligible for vaccination]’. The majority of these unvaccinated admissions is middle-aged men (median age: 54), with ‘only 29% of these with any number of co-morbidities’. By contrast, the ‘fully vaccinated’ and/or ‘boostered’ patients were overwhelmingly elderly (median age: 71), with three out of four belonging to high-risk groups. (p. 9).
Sidenote: there’s a reference to a pre-print study (‘Patient trajectories among hospitalised COVID-19 patients vaccinated with an mRNA vaccine in Norway: a register-based cohort study’, by Robert Whittaker et al., which you can find here), which the IPH uses to bolster the above claim. In my reading, it’s a problematic piece for two main reasons: on the one hand, the authors looked at an inverse share of admissions (3% fully and 8% partially vaccinated vs. 89% unvaccinated) while, at the same time, they investigated the period from 1 Feb. through 30 Sept. 2021. That means that the reversal in admissions from weeks 41-49 (when vaccinated admissions exceeded unvaccinated ones) don’t appear in the paper, on the other hand. Hence the (still) contradictory conclusions (my emphasis):
We observed no difference in the LoS [length of stay] for patients not admitted to ICU, nor odds of in-hospital death between vaccinated and unvaccinated patients.
Conclusions: Vaccinated patients hospitalised with COVID-19 in Norway have a shorter LoS and lower odds of ICU admission than unvaccinated patients. These findings can support patient management and ongoing capacity planning in hospitals.
I shall discuss this paper in a separate post, for here it suffices to note that the IPH risk assessment (p. 8) uses this paper on hospitalisations from 1 Feb. through 30 Sept. 2021 to support its claims about the vaccination status of these admissions in weeks 47-50, as the screen shot below clearly shows (I’ve highlighted this in yellow; table 1 in that paper is on p. 19 in the pre-print):

Now, as I said before, I’m not a medical doctor or epidemiologist, but I’m able to read numbers and dates, and I fail to understand how data on 1 Feb. through 30 Sept. 2021 as per the referenced pre-print has a bearing on weeks 47-50 that isn’t historical, i.e., problematic if referred to without context.
In my world, these discrepancies matter, and they matter a lot in light of the recent ten weeks (40-50): in that period, the numbers of ‘fully vaccinated’ admissions (both ‘regular’ and ICU) have all but exploded and risen by around 300%, as opposed to an approx. 11% increase among the ‘unvaccinated’ (preliminary data here, I’ll have more on this in a future post as explained above; my ‘sources’ are the IPH’s weekly updates).
Vaccine Uptake
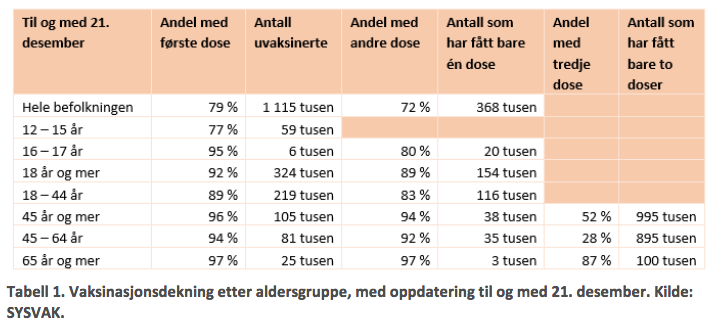
Then there’s table 1 (p. 11), reproduced below, which emphasises the above point: vaccine uptake in the most affected age cohorts (45+) is north of 94% by now, hence all data on hospitalisation, ICU admission, and death must be considered in light of these very high shares. Do note that in that particular group, slightly more than half of all Norwegian residents has received a third, or ‘booster’, jab by now. (Table 1 gives the shares at 52% but breaks it down to 28% among 45-64 and 87% among seniors.) That would be another aspect that should be in the above considerations by the IPH on what the vaccines do and what kind of role(s) they may play in all of this.
My take here is that the rapid roll-out of the booster jabs is very much ‘distorting’ the trends on hospitalisations (‘regular’ and ICU admissions). I would further point to the fact that we don’t know much about the efficacy and longevity of the third jab, but given the high uptake in Norway, this is probably as close to a natural experiment as we will get—and in a few weeks, we shall learn how much and for how long a third jab of the same vaccine (that many experts said didn’t afford protection against Delta) will help the vaccinees now.
I suspect that protection might wane even more rapidly than against earlier strains, hence the ‘fully vaccinated-and-boostered’ group will run into serious problems within weeks, if the rates of ‘breakthrough infections’ (roughly 3 out of 4) with Omicron coming out of comparable places like Canada (here) and Denmark (here and here) are any indication.
On p. 12, there’s a section entitled ‘Short-term Projections’, is introduced by the following statement (emphasis in the original [!!!]):
The National Institute of Public Health is trying to estimate the disease burden in the coming weeks based on projections of developments observed in recent weeks. These projections do not take into account the Omicron variant. See Chapter 3.6 for long-term scenarios for the omicron variant.
In other words: there’s no need to continue reading the updated risk assessment. We’re back to ‘mathematical modelling’, hence it’s safe to assume you and I can also check in with a soothsayer to determine future outcomes at this point.
That said, there is now a large section—in the Covid-19 risk assessment, mind you—on the likelihood of an influenza outbreak in the coming weeks, as shown in figure 12 (p. 13).

On Omicron (pp. 16-24)
There’s a lot of ‘background’ information, which I’ll spare you—for the one reason spelled out on p. 18: ‘The importance of these early reports from South Africa for Norwegian circumstances is hard to estimate’, mainly because (I’m not making any of these below points up, by the way):
Most infections occur in previously non-infected individuals; hence they haven’t had time to develop serious illnesses;
Many of those infected are young, i.e., people who quite likely won’t develop serious illness compared to elderly patients;
There’s more testing these days, hence there are likely more ‘cases’ who wouldn’t have been identified otherwise (irrespective of symptoms);
Unvaccinated individuals [who test ‘positive’] may have had Covid-19 before and may already have natural immunity;
South Africa experienced three big waves already and most vulnerable people may have died already, hence fewer serious cases can be expected;
In Gauteng Province, the Christmas holiday began a week earlier, which may have arrested the outbreak.
There are two brief sections on the UK and Denmark, respectively, which both conclude that it’s ‘too soon to tell’.
And why, pray tell, might the IPH’s assessment be thus? I’m glad you asked—the UK data is from 15 Dec. (see footnote 15 on p. 18) and the Danish one from 21 Dec. (as per footnote 21 on p. 19) , but the data cut-off date is similarly 15 Dec. (see here).
By now there are certainly other estimates, among the better ones is certainly Chris Martenson’s over at PeakProsperity.com. Still, the main issue anyone pushing a third, fourth, or any additional jab, for that matter, should be concerned about is vaccine efficacy vs. Omicron, and here the IPH is either off the reservation or simply disingenuous, noting (on pp. 21-22 (my emphases, references omitted) that whatever vaccine protection may be there,
these [protection] levels fall significantly within a few months, and the first data indicate that the same will happen after a third dose…
A booster jab of an mRNA vaccine provides a significant increase in neutralising antibody levels to the variants of concern, including omicron…antibody levels after booster vaccination decrease after some months [fn. 42], and thus probably also the Omicron-specific neutralising capabilities [of the jabs].
If one follows footnote 42, one reaches a pre-print paper by Wilhelm et al. (see here), of which a more recent, or updated, version was available since 13 Dec., i.e., the IPH didn’t compile this part based on the most current version. Be that as it may, that paper by Wilhelm et al. concludes
Our in vitro findings using authentic SARS-CoV-2 variants indicate that in contrast to the currently circulating Delta variant, the neutralization efficacy of vaccine-elicited sera against Omicron was severely reduced highlighting T-cell mediated immunity as essential barrier to prevent severe COVID-19.
I think the one ‘saving grace’ of the IPH’s risk assessment is that they also say, however implicitly, that they don’t know. While the IPH admits that ‘much is unknown’, their conclusions are ominous (p. 24, my emphasis):
It is important how the variant will behave in a population such as that in Norway [i.e., 90+ % jabbed]. If immune evasion is the main problem, there will be many more in our thoroughly vaccinated population who can potentially become infected and carry the infection further. Fortunately, the vaccinated probably still good protection against severe course.
So, there you go—the word is out.
What does the risk assessment mean?
First, I still don’t get it why the IPH and the Norwegian gov’t (as well as many other Western gov’ts) are still pushing booster jabs as Christmas presents—the IPH admitted they don’t know.
Second, the entire booster campaign is a quite gigantic sub-experiment, and we’ll probably know in a couple of weeks—mid-January, as far as I guess.
Third, this is all political posturing: everyone is super-concerned about Omicron, hence the IPH must show to be doing something, hence these breathless reports based on somewhat outdated data and modelling.
Fourth, the above third statement also applies to the irresponsible politicians who won’t call out this pile of steaming horse manure.
Finally, what’s the overall use of these reports? I would say that gaslighting by (legacy) media is their current MO. Gaslighting by politicians who try to avoid responsibility for their actions is also a given. The main problem here is the deterioration of the IPH as a useful agency to guide public policy, and as such, at least with the jabbing against (with) Omicron fiasco in-the-making, the IPH appears well on track to join its peers.
You can see these issues, in particular the last one, on display in the report’s conclusions on pp. 25-26 (emphasis in the original):
We consider that it is likely that the omicron variant will give a new wave of the epidemic from January because the variant has a greater dispersal ability. The size of this wave is uncertain; it can be very large with up to several hundred daily admissions. The size will depend on the variant’s ability to spread, vaccination support and vaccine effect, effect of infection control measures and effect of the population's self-selected behavioral changes
There you have it: we don’t know much, we hope that what we’ve done so far (jabs) will continue to work, and, failing that, that any of the non-pharmaceutical interventions will work.
Bottom line: brace for impact, if you’re inclined to believe in the authorities’ fear porn. If that is indeed so, I’d have a bridge to sell to you, too.
"...Our in vitro findings using authentic SARS-CoV-2 variants.."
"Authentic"?
Regarding the relentless booster push for the holiday season: countries might have a bunch of vaccines that are expiring Dec. 31? https://www.lewrockwell.com/2021/12/vasko-kohlmayer/this-is-what-a-reader-wrote-me-about-the-vaccine-madness-in-ireland/