


Covid-19 in Norway: Authorities Recommend Lockdown because Omicron might Harm the Vaccinated
The IPH is out with a new assessment, and it expresses concern over Omicron ‘among a highly vaccinated population'--a new lockdown because of vaccine uptake is in the making

I wanted to write something about last weekend’s happenings in Covidistan, but then this happened: the Norwegian Institute of Public Health (IPH) just published an ‘updated Covid-19 risk assessment with respect to Omicron’, so, here goes.
One brief note: this report isn’t available in any other language than Norwegian; if you don’t read Norwegian but wish to go through it, let it be known that, while far from perfect, Google Translate renders an o.k. service in this regard. [EDIT: I spotted some minor issues, typos, etc after posting, hence some corrections are in this post now; kudos to readers Barry and Billy!]
This is from the IPH’s ‘news’ website entry
The situation is increasingly serious. The number of detected cases of Sars-CoV-2 infection is increasing rapidly and is followed by an increase in admissions.
Hospitals, nursing homes, GPs and emergency rooms are experiencing an ever-increasing burden as a result of sick patients, increased sickness absence among health personnel and less access to temporary staff from abroad.
The Omicron variant is in the process of establishing itself in Norway and will soon become dominant. This will significantly increase the spread of infection.
If you’re not cowering in fear, hiding under your blanket while crying, the ‘news’ update continues like this (my emphasis):
There may also be an influenza epidemic from the end of December or in January, but this can be slowed down by the measures against the Covid-19 epidemic [note the use of the word ‘epidemic’, instead of ‘pandemic’].
There is an urgent need to curb the Covid-19 epidemic with significant measures so that the omicron variant does not cause an epidemic wave that places an enormous disease burden and completely overloads healthcare service. Their purpose is to reduce and flatten this wave [when, where, and how often have we heard that one before?].
Vaccination also reduces the risk of a serious course with the Omicron variant, even if the protection against becoming infected is reduced [more on this below].
There’s a bit more boilerplate talk about how healthcare-related problems may spill over into other sectors of society and economy, as well as a call to all actors to ‘review their contingency plans’.
With these preliminaries out of the way, let’s take a look at the IPH’s report.
The document has four main sections:
Covid in Norway
Omicron
Projections for December and January
An overall assessment.
We shall look at all of these, and at the bottom of this post you’ll also find a brief estimate of mine about what will most likely happen next.
Covid in Norway (pp. 6-16)
Since September, there’s increased pressure on healthcare services, mainly due to respiratory diseases. Affecting the entire country, these pressures are due to ‘the spread of the common cold, esp. Rhinovirus, Parainfluenza Virus, and RS Virus’ (p. 6).
In the same period, the number of Covid ‘cases’ has risen sevenfold, we learn further below (p. 7), from c. 3,000 in week 41 (11-17 Oct. 2021) to more than 20,000 I week 48 (29 Nov.-5 Dec. 2021). Sounds dramatic, but it is also explained that this ‘may be due to the fact that a smaller proportion of cases are registered as the population has largely moved from laboratory-confirmed [PCR] tests to [rapid antigen] tests, which are registered only if you take a [PCR] test afterwards’. As a consequence, the assessment concludes that
‘the number of registered cases is therefore now a less reliable indicator’.
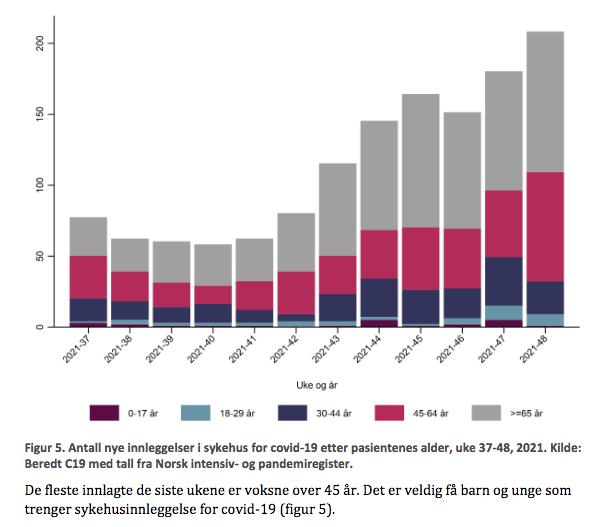
Throughout, the report is heavy on illustrations and very light on actual data. Take, e.g., the below example (fig. 5, p. 8), which shows the ‘number of hospitalised patients with Covid-19 as main cause from weeks 37-48 [20 Sept.-5 Dec. 2021]’ with the below text stating that the majority of inpatients are 45 and older’.
There is a bit of relevant information below (p. 9), which emphasises, perhaps inadvertently, that the main problem—area of concern—is Norway’s capital, Oslo, which easily outpaces the rest of the country in ‘cases’, admissions, and the like.
Curiously, we also learn that ‘in weeks 45-48 [8 Nov.-5 Dec. 2021] four out of ten hospitalisations for Covid-19 as main cause occurred among the unvaccinated’. Among the ‘unvaccinated’ inpatients, the median age was 53, among the ‘fully vaccinated’, it was 74 years; among the latter, three quarters also belonged to groups with medium or elevated risk. (pp. 9-10).
Sidenote: I pointed this out at the time (see here for week 47 and here for week 48), and while I appreciate confirmation of my reading, this assessment stands in direct contradiction to the IPH’s last two weekly assessments. This confirms that my criticism about the IPH monkeying around with the numbers was correct.
Moving on to table 10 (p. 11) on ‘vaccination uptake’, we learn that 79% of the entire resident population has been vaccinated with at least 1 dose. Vaccine uptake has been highest among the age brackets 45+, with 94-97% vaccination rates.

Like my next-door co-worker said yesterday, ‘the problem is with large groups of immigrants in Oslo who refuse to get jabbed’ (incidentally, at the same time, he stated that while he took two jabs, he’d ‘rather get Covid than take third one’). Make of my co-worker’s rant what you will, but the report also outlines this on pp. 11-12, noting considerably lower ‘vax uptake’ among Poles, Romanians, and Latvians (all 40% ‘fully vaccinated’), Lithuanians (43%), Somalis (54%), Russians (58%), Eritreans (60%), Syrians (66%), Iraqis (68%), and Pakistanis (75%),.
This section concludes with a ‘short-term projection’ (p. 12), which is my ‘favourite’ bullshit part of this part, as the disclaimer reads as follows:
The model does not take into account the effect of new measures that are introduced, behavioural changes that can be expected due to increasing infection rates over time, or the Omicron variant.
In other words: someone made this projection before we wrote the report, and while it is therefore useless, we included it anyways.
‘Other respiratory infections’ (pp. 13-16)
On p. 14 we learn that there’s almost no-one with influenza in Norway (28 positive tests out of 15,017 in week 48, i.e., a test positivity rate of .21%), which caused nine hospitalisations so far. It’s also noted that most RS Virus infections concern kids below age 5. Oh, they also use the same illustration (fig. 15, p. 15) as in last week’s report.
The Dangers of the Omicron Variant (pp. 17-27)
This is the largest section of the report, and it is also the most troubling one—but not because of Omicron. So far, the IPH admits to ‘outbreaks in a number of municipalities’ while cautioning against future efforts of contact tracing, stating (both on p. 18), that
as the variant becomes more widespread, the Institute of Public Health will have less detailed information on transmission routes for all cases with the proven Omicron variant.
I’m glad we got the helpfulness of contact tracing efforts out of the way (which the government re-introduced for restaurants last week, albeit ‘only for those clients who agree’ to share their data).
The report then moves on to state (the perfectly obvious) fact that ‘severity of the diseases can be different for vaccinated and unvaccinated’. While there’s a number of references (esp. to a preliminary observational study from South Africa), the main highlight is on p. 19, in the section ‘Effects of Vaccination’ (references omitted; my emphases):
If more severe course of the disease is observed in vaccinated people, it is difficult to determine whether this is due to the virus’ virulence or immune escape. Similarly, reports of milder disease in vaccinated individuals must be interpreted with caution. In that case, it is not a given that the variant will give milder disease also in the unvaccinated.
There is some speculation about how (far) continued efficacy of vaccine-induced T-cell activation may or may not help against Omicron, but the conclusions (ibid.; my emphases) speak for themselves:
Basically, it is uncertain whether Omicron leads to more or less severe disease compared to Delta, but [if it did so] this would have been discovered by now. We also do not know whether Omicron affects different age groups differently compared to Delta.
Omicron thus causes either as serious or less serious disease compared to Delta in vaccinated persons who had previously had Covid-19 and in unvaccinated.
In other words: we don’t know whether Omicron is as bad as Delta; if so, we’d have heard about it by now, and we also don’t know if Omicron affects the ‘vaccinated’ and the ‘unvaccinated’ in the same way across any of the age cohorts.
It would be nice to actually know about these issues, in particular the ‘vaccination differential’, right?
Leaving aside ‘unclear’ evidence from the UK, let’s see what the IPH has to say about ‘vaccine efficacy’ against Omicron (pp. 20-21; references omitted; emphases mine):
Several in vitro studies with sera from vaccinated showed reduced [vaccine] neutralisation against certain variants and mutations. Nevertheless, two doses of mRNA vaccines [by Pfizer/BioNTech and Moderna, that is] produce such high levels of neutralising antibodies that in most cases it will be sufficient to neutralise all known viral variants of concern despite reduced vaccine efficacy. Unfortunately, these antibody levels drop significantly within a few months, and it is likely that the same will happen after a third dose [or this will happen much faster].
Theoretical analyses [sic] suggest that Omicron features significant changes in its receptor binding-domain while another analysis predicts that the variant will not completely escape neutralising antibodies.
There are two more paragraphs of equally telling, if hardly legible, ‘officialese’ (same sources etc. as above):
The study of a Covid-19 outbreak caused by the Omicron variant [that would be the Oslo Omicron Outbreak] suggests that young and middle-aged adults vaccinated with two doses of mRNA vaccine a few months earlier may be at high risk of infection and illness with Sars-CoV-2.
The first study of vaccine efficacy [against Omicron] from the UK indicates that protection after vaccination is about 20-30% lower Omicron compared to Delta.
Sidenote: that UK study
Let’s linger, for a moment at least, on the ‘first study of VE from the UK’, which can be found here. In that study, a pre-print (i.e., not yet refereed), the main problem is with the study design and comparisons.
To provide, really, all that one needs to know about this study, here’s the main design flaw:
‘Vaccine effectiveness was also assessed for both primary courses followed by a [Pfzer/BioNTech] booster for the period 1 week and at least 2 weeks post vaccination. Comparison was to unvaccinated individuals to estimate the absolute effectiveness of vaccination against Omicron and Delta variants.
Numbers were too small to estimate vaccine effectiveness with [Moderna] as either a primary course or a booster. (p. 5)
They only really looked at ‘fully vaccinated’ or ‘recently-boostered’ individuals, and the findings aren’t promising (pp. 5-6). Generally, VE ‘was lower for Omicron compared to Delta post vaccination at all time interval investigated.’ There are some differences deriving from the ‘vaccine’ used (AstraZeneca is ‘weaker’ in this regard than the mRNA jabs), but one fact is obvious: VE drops rapidly, including—in spite—of a ‘booster’; there appear only brief upticks in VE for 2-9 weeks after getting ‘boosted’.
Here’s the gist from the discussion (my emphases):
Our findings show that vaccine effectiveness against symptomatic disease with the Omicron variant is significantly lower than with the Delta variant. We are unable to determine protection against severe forms of disease due to the small number of Omicron cases so far and the natural lag between infection and more severe outcomes.
Despite the low effectiveness in the longer intervals after primary vaccination [that would be jabs 1 and 2] shown here, moderate to high vaccine effectiveness against mild infection of 70-75% was seen in the early period after a booster dose of Pfizer following either AstraZeneca or Pfizer as a primary course.’
Further below, reference is made to the problem of earlier (older) vaccinees who received the AstraZeneca jabs, as opposed to younger (under 40 years) who received any of the mRNA jabs; in addition, recently-boostered individuals further skew these findings (p. 7):
High vaccine effectiveness against Omicron 2-9 weeks after the second [and/or third] dose of Pfizer is likely to be primarily among recently vaccinated young adults and teenagers.
There is nothing in this pre-print that indicates any data beyond 2-9 weeks after the second or third jab. And this is against Delta, not against Omicron, mind you.
Let’s return to the IPH’s assessment (p. 21, my emphases):
Omicron has a greater spread potential than Delta, and the main reason is that Omicron to a greater extent bypasses immunity after infection or vaccination. Given wide-ranging vaccine uptake among our population, there is a high possibility that they [the vaccinated] can be infected and further contribute to the spread of infection. Fortunately, the vaccinated probably still have good protection against severe outcomes [if infected].
There you have it. It’s immune escape writ large, with the IPH admitting that they don’t know how this affects Norway’s highly vaccinated population.
In other words: the stringent new measures announced yesterday (13 Dec. 2021, on which you may see primer here) are implemented because of the high vaccine uptake.
If this isn’t an admission of vaccine failure, I don’t know what is (or could be).
This brings us to the IPH’s modelling that drove the government’s decision to (partially) lockdown the country again. Earlier today, media was full of fear-inducing claims of ‘up to 300,000 infections around New Year’s Even’ (e.g., Aftenposten on this).
What’s the basis for this? I’m glad you asked, here’s the same report (pp. 21-22):
Huge uncertainties aside, preliminary data suggests Omicron spreads as fast as elsewhere, i.e., with ‘a doubling time of 2-3 days’.
If this spread continues, it is estimated that Omicron will reach 50% of all cases in Norway between 18-23 Dec., yet everything beyond this estimation is ‘too uncertain to tell’.
Yet, based on ‘simplified modelling’ [doh], the following assumptions are central:
Omicron is just as serious as Delta
Vaccines protect against severe disease, but
much less well against infection (transmission)
‘without [assuming] any effect of the measures announced on 8 Dec.’
If these conditions are met, and only *then*, ‘the number of new daily infections with (of) Omicron in three weeks [i.e., New Year’s Day] may be between 90,000 and 300,000’.
You see, it’s easy: the media assumed the rather very unlikely worst case, the government ‘jumped’, and there you have it.
For fun’s sake, there’s also quite a laundry list of ‘limitations’, which include (and I’m not making this up either, it’s on pp. 22-23, with light edits for clarity and concision):
Great uncertainty about how fast Omicron spreads and how many are infected
No seasonal variation and no regional differentiation
Age distribution of those infected based on the proportion of infected in recent weeks and not on contact structure (i.e., different patterns of contact apply to different age groups)
None of the measures adopted on 7 Dec. 2021 are considered
No consideration of ‘imported’ infections
No consideration in vaccine uptake or effect over time
Great uncertainty around all parameters
Both variants [Delta and Omicron] are modelled without reference to each other
Assumption that protection against infection after a booster dose is the same as shortly after two doses
Assumption of vaccine-induced protection against serious illness is assumed to be the same for Omicron as it is for Delta
Uncertainty about severity per infection for Delta
The model [which one, there are two, but it’s not said] assumes a random mixing (distribution of the virus variant) in the entire population, which probably increases the risk of rapid spread of Omicron
This list of ‘limitations’ is so comprehensive, it makes a black hole look like an afternoon picnic in a park. My personal favourite is ‘great uncertainty around all parameters’—what’s your’s?
There’s a number of modeling visualisations there (pp. 24-25, with methodological explanations on pp. 26-27) that all project Omicron to surpass Delta in a few weeks. The measures announced last week are supposedly reducing the spread by about 15%, by which is meant that they may push that point in time a few days into the future.
Thus, let’s briefly consider the final two parts of the assessment.
Covid-19 Risks in Norway in Dec. 2021/Jan. 2022 (p. 28)
The situation is serious. The number of detected Covid-19 cases is increasing rapidly and mirrored by admissions. There are no sure signs that the situation is about to flatten or turn around.
Curiously enough, from late September 2021, weekly hospitalisations for Covid-19 have increased from 60 to (week 39) to 144 (week 44) to over 200 (week 48), which were mostly driven by ‘fully vaccinated’ admissions. As of this writing, hospital admissions for Covid-19 as main cause are higher than 300 (week 49). Still, further increases must be expected in the coming weeks, ‘especially in the east-central part of Norway’, i.e., in the capital region with its large vaccine-hesitant immigrant population.
Failure of last week’s measures to show any measurable effect is acknowledged, hence the government announced new measures on 13 Dec. Oddly enough, it usually takes ‘two weeks to flatten the curve’, but nevermind.
Yet, the IPH’s assessment gets curiouser and curiouser. To ramp up the fear factor, there is this statement in the middle of the assessment (my emphasis):
The risk of hospitalisation is many times higher for the unvaccinated than for the fully vaccinated across all age groups. Among fully vaccinated people under the age of 65, there are few admissions and no definite signs of weakened protection against serious illness. Unvaccinated people over the age of 45 have a particularly high risk of hospitalisation
While there is some truth to this, it’s clearly a gross exaggeration, as the IPH’s own numbers (whatever they are worth) show: the main problem is fading vaccine efficacy, which is now compounded by the risks posed by Original Antigenic Sin. For seven weeks now—from early October onwards (week 41)—hospital admissions of ‘the vaccinated’ have outpaced those of ‘unvaccinated’ patients, wth the former now caught between a proverbial rock (fading VE) and a hard place (OAS). Even the most recent data (from week 48) shows this quite clearly, especially as the age distribution, which is done without reference to vaccination status, reveals.
For those not fully cowering in fear crying for their cuddly blankets, there is still more: there’s talk about a significant influenza epidemic hitting the country ‘normally around the end of December’. This, of course, elevates the risk of overburdening healthcare providers (GPs, family doctors, clinics, and hospitals), with many of them already hard-pressed ‘because of many seniors hospitalised for respiratory infections other than Covid-19’.
This situation is further compounded, the assessment continues, by ‘similarly infected healthcare workers and their children, lower thresholds for sick leave and self-isolation rules, and the impossibility of importing qualified personnel from abroad’.
On top of these issues mainly unrelated to Covid-19, there is, again, the following admissions (pp. 29-30; my emphases):
Omicron is more transmissible than Delta, in particular due to reduced vaccine efficacy against infection and transmission. Protection is perhaps offered against serious illness [though nothing about death is said, which is hardly surprising given that 4 out of 5 people who die of Covid-19 in Norway were fully vaccinated]
Omicron will be the dominant variant in Norway within December 2021. Still, we don’t know how this variant will affect a highly vaccinated population that is already affected by a big Delta outbreak…
Omicron is highly likely to exacerbate already-existing problems caused by illness, the overworked healthcare system, and in the wider society on top of Covid-19.
Recommendations by the IPH (pp. 30-32)
I’ll keep this short, as the Norwegian government has already announced new measures yesterday evening. Here are the main points (again, my emphases):
Vaccine-induced protection against (re-) infection is gone after a few months. It looks like protection against serious illness lasts longer. This means that both vaccinated and previously infected after some time can become reinfected and spread the disease [again]. Thus, while vaccination with the current vaccines alone cannot keep the spread of infection under control, these [current vaccines] can reduce Covid-19’s burden.
Furthermore,
there is an urgent need to slow down the epidemic so that Omicron does not cause an epidemic wave…completely overruns healthcare services. The purpose [of any measures] is to reduce and flatten the curve [haven’t heard that one in a while, have we?]. New measures must last for several weeks until one will see a clear reduction in the burden on healthcare service, and then it shall be reconsidered…
The implications of immunity after infection in vaccinated people must be examined. Since the virus will be with us forever, a long-term strategy must be drawn up to deal with an endemic disease that will probably follow this winter wave.
At least there’s some hope about learning from (past) experience, hence not all is lost.
Brief comment
The main take-aways from the IPH’s assessment are:
While many countries are in ‘lockdown’, either for all or ‘only’ for ‘the unvaccinated’, Norway appears to be ‘one step ahead’ of the curve here. The government announced a set of stringent measures on 13 Dec. 2021 because immune escape and—perhaps even Original Antigenic Sin—are becoming an ever-bigger problem that, at least in Norway, is becoming impossible to hide.
There were some hate-filled comments about ‘the unvaccinated [who] prolong the pandemic for everyone else’, as the below example shows. This one, e.g., appeared a few days ago in Bergens Tidende, much to the disgrace of its author, Morten Mkysvoll (who mentions that it’s a civic duty to get jabbed, hence there’s no need to force-jab if everybody just rolls up his or her sleeves and takes one for the team).

Seen in this light, the IPH’s admission that any measures are to be taken because of the ‘fully vaccinated’ is remarkable (even though I remain wary that they actually intended to say so).
In the end, it remains to be seen how far the population is willing to participate in this charade. Already, the PM has admitted that he cannot ‘see a way out of the situation’ and that the government ‘cannot guarantee that the measures will curtail the spread’.
The spread of disease, mind you, is but one aspect, with long-term damage done to the healthcare sector over the past decades being the elephant in the room. Yes, current situation is a problem, but the larger issues are decades-long under-investment in public healthcare, compounded by the inability to simply import qualified workers from abroad right now to paper over these structural problems.
Thus, Covid-19 appears to be a ‘catalyst’, i.e., a sign that our current societal and economic configuration is the root cause of this mess. Omicron in particular may be the proverbial straw (-man argument) that finally breaks the camel-named-society’s back, mainly because of fading vaccine efficacy and the unknown risk potential of a ‘new’ variant spreading among an overwhelmingly vaccinated population, something known as Original Antigenic Sin.
What, then, is to be done?
I suppose that if you’re in Norway and not (yet) vaccinated, it’s safe to assume it’s better to stay unvaccinated. Mind you, that entire report barely mentions ‘the unvaccinated’, with the one notable exception that vaccine uptake has been particularly low among immigrants (pp. 11-12).
I do get this feeling that the ostensibly left-of-centre government is setting up the immigrants as the scapegoat for these new measures, which are hugely unpopular, in particular the limitations on the number of invitees to private Christmas parties and the prohibition on alcohol sales in bars, restaurants, and the like.
It remains to be seen if the sheep-like adherence of Norwegians to any governmental ‘recommendation’ will continue well into the future. If my co-workers’ attitudes are any guide, there will be less compliance going forward.
This has become already too long, hence I shall stop now and discuss the government’s new measures in a separate post.
Depressing but good article as always.
I’m convinced that this is all to do with digital currency, the vaccine being the gateway to the vaccine passport and so forth.
What I don’t get is that they could implement the same system using the much safer pfizermectin. I get that you cant hide a pill under your tongue but not a vaccine. I get it. But still. They could say that they have to issue the magic pill from a central authority. And they have to do it every six months in case more deadly variants appear etc etc.
But there is this push to vaccinate. And they know it’s dangerous. Of course they do. It’s evil.
Here is a promise I would bet my home on: there will never never never be any protests in my town against the vaccine program. I can back this up by showing you all the shops that happily excluded the unvaccinated before it was law!
This is a rich town in a rich part of Germany and these are the most compliant of the compliant.
And guess what ? I am wrong. Dead wrong. Last night there was a huge protest.
You must understand that the worst thing to be if you are German is to be a Nazi. The second worse thing is to be called a Nazi. And these people are risking that. That’s a big deal for a German. People have had enough.
They are scared, and with a good reason. They highly suspect that the only bullet in the chamber, the vaccines, does not work at all. And we have a highly COVID-naive population, with about 3% ever infected
And the suspicion of OAS has been growing everywhere in the last two months. For example in the British reports and the Israeli airport study.
I think it is going to be much worse now than last year.