


Covid in Norway: Numbers from Week 8 show hospitalisations for 2 dose-recipients are up 760% since 6 Oct. 2021, and +1,975% for 'boosted' since 6 Dec. 2021
Injection failure too big to hide, more comparative insights on risk ratios, hospitalisation, ICU admissions, and the like show drastically higher risks for 'all-cause injected'--*sigh*

Again, I’m a bit late on this one, but there’s a quite plausible set of explanations for this: on the one hand, the Institute for Public Health (IPH) only came out with the report a day later (that would be Thursday, instead of Wednesday), and then there’s quite a backlog of what I wanted to write about on Covid in Austria and Norway, specifically, that also had to wait the more current news from last week.
Be that as it may, for comparisons I’ll simply link to both the numbers for week 7 (14-20 Feb. 2022, original file here, my piece is here) as well as my three-part series on the most recent injection-related adverse events report by the Norwegian Medicines Agency (pt. 1, pt. 2, and pt. 3), which further includes notes on possible fourth injections, female reproductive issues, and severe adverse events.
That said, let’s have a look at the Institute of Public Health’s (IPH) update for week 8. As always, I’ll provide you with the page numbers of sub-chapters and quotes, with all emphases mine.
As I mentioned in the last dedicated post, keep in mind that these are ‘Covid updates’, but they regularly exceed 80 pages and contain so much, much more information, which this week also includes a neat global comparison of cases and deaths (both absolute numbers and rates per 100,000), lethality, and data on injections for week 8 (pp. 79-80).
Executive Summary (pp. 3-4)
Hospitalisations for Covid-19 as main cause are still rising and reached 450 in week 7 (up from 430 in week 7), which corresponds to a 14% increase week-over-week. The pace of increase has slowed, though, for there were 313 such admissions in week 6 (week-on-week increase of 27% from week 6 to 7), but keep in mind that hospitalisations have risen 44% in the past two weeks. One of the main benefits of the Norwegian data is that we also learn the overall number of new admissions, which in week 8 stood at 910, which is to say that hospitalisation for Covid-19 was given as main cause in 49%.
‘The number of new admissions per 100,000 inhabitants was highest in the age group of 85+’, which, again, isn’t a surprise. Here’s a breakdown of hospitalisation incidences by age group, incidence, and numbers from both week 8 (and week 7 in parentheses):
85+: incidence/100,000 = 77.5, n = 91 (53.6, n = 63)
>1: incidence/100,000 = 64, n = 34 (48.9, n = 24)
75-84: incidence/100,000 = 35.4 (29.2)
65-74: incidence/100,000 = 14.4 (13.9)
55-64: incidence/100,000 = 8.5 (7.1)
Among all other age cohorts, hospitalisation incidences ‘was relatively stable or declining’.
Obviously, hospitalisations for Covid-19 ‘as main cause’ are still rising, and they were rising even more last week due to reporting delays. Note that this is really telling—Omicron (whatever variant) is supposedly ‘mild(er)’ than previous strains, but look at these numbers: hospitalisations for Covid-19 were never higher, and the sheer number of people on sick leave is also elevated (cue my daughter’s kindergarten with reduced opening hours due to staffing issues for four out of five workdays last week).
Brief comment: I decided to include the >1yo bracket in the above listing, for last week they said it was an outlier or the like, but the incidence is still elevated. Note further that the IPH doesn’t list the number of individuals consistently; one more thing to mention is that they also (upwardly) corrected the above incidences, i.e., as time passes, the numbers become ‘more correct’ (I’m mentioning this as the incidence rates given in week 8 are all a bit higher than in week 7). Note further that the ‘disclaimer’ about the >1yo is still there, which holds that ‘admission [of infants] is generally short-lived’.
Injection status was known in 488 cases (note here that ‘only’ 450 admissions occurred due to Covid-19 as main cause; 488 out of 910 comes down to 54% of the total). Of these, 119 (24%) were ‘unvaccinated’, 86 (18%) had received two doses, and 268 (55%) were ‘vaccinated with three doses’ (by comparison, these numbers stood at 87 (26%) were ‘unvaccinated’, 58 (18%) with two doses, and 175 (53%) with three doses in week 7).
Last week I spoke of ‘alignment’, by which I meant the eventual (temporary) equilibrium between hospitalisation rates and injection status: 53% of the overall population has received three doses (as of week 8), and uptake has been incredibly high among all age brackets 45 years and older (81% of all residents over 45, and 65% of all residents over 18)
I’d tentatively hypothesise that the younger the ‘vaccinee’, the less overall risk for a Covid-related and/or injection-related admission. That said, while I therefore doubt that we’ll see rates in perfect alignment with injection uptake, I suppose that we haven’t yet reached the ‘ceiling’ of Covid-related hospitalisations.
As mentioned last week, this public health policy disaster was entirely expectable, and to deflect blame given the relationship between cause and effect, the IPH notes:
Vaccinated patients had an overall higher median age and a high proportion [of them] has conditions amplifying their risk [har risikofaktorer] that lead to increased risk for a severe course of Covid-19 relative to the unvaccinated.
Plain English: vaccine failure, expressed in so many words, for this is nothing but a rather carefully worded statement that the final sales pitch—that while not 100% effective, the injections would at least provide (some) individual protection from severe disease—has become untenable.
ICU admissions and deaths are both rising, with the former being quite telling: 38 ICU patients (week 7) and 35 (week 8, but this number is subject to adjustment, i.e., it’ll rise, too), and here we also see the drastic nature of the Omicron wave: in weeks 4-6, there were 15-19 new ICU admissions, and now in weeks 7-8, it’s twice that number.
Covid-associated deaths stood at 57 in week 8, up from 48 in week 7 (with the same caution, i.e., that number will be ‘adjusted’); the median age was 84. The IPH also notes that all-cause mortality ‘was normal in the past two months, including persons 65 years of older’. All-cause mortality is said to have been within the long-term range, with the exception of weeks 43-45 and 47-51 in 2021.
Last week I noted that the case rates may be a data artefact, and I suspect I was correct: the number of registered positive tests (PCR and antigen rapid tests) remained at virtually the same level (100,722 in week 8, as opposed to 100,713 in week 7), which means that the Norwegian testing data is useless at this point as it won’t tell us anything about the epidemiological trajectories. We shall thus stick with the hospitalisation records, which are much more reliable in any case.
Final points here—injection uptake: as of 27 Feb. 2022, 78% of the entire resident population has received at least two doses; in the 16+ bracket, the share is 91%, and in the 18+ bracket, it is 91%. Of the entire resident population, 53% has received a booster injection, even though this breaks down differently across the various age brackets, with 89% booster uptake among 65+, 81% for those over 45, and 65% for those over 18. Injection uptake has crested, there is virtually no significant change among these numbers from last week.
Among high-risk groups aged 18-64, injection uptake stood at 81%, among those in the same age bracket with moderate risk, it stood at 73%.
Cases and Testing provide Perspective
First, some perspectives, courtesy of fig. 4 (p. 11), which plots the test-certified number of positive ‘cases’ (blue line) vs. the number of hospitalisations for Covid-19 as main cause (red line).

This figure is very much misleading, for we just noted that the number of reported cases in week 8 is virtually indistinguishable from week 7. There’s no adjustment that I know of with respect to the underreporting factor (i.e., we don’t know how many people test positive for Sars-Cov-2 and don’t report it online). Note further that hospitalisations lag positive tests by about ± 3 weeks, hence while the peak of the ‘testing wave’ may have arrived by now, it’s entirely predictable that hospitalisation will increase even more before that wave breaks. At this point, I honestly don’t know what the rationale behind plotting these two curves in the same figure is: dear IPH, what are you doing?
Another way to show the problem of ‘Covid-19’ or ‘indirect Covid’ (the injections) contributing to a rather grim winter-and-spring season 2021/22 are the rising incidences for the 65+ age brackets, as shown below in Fig. 6 (p. 11).
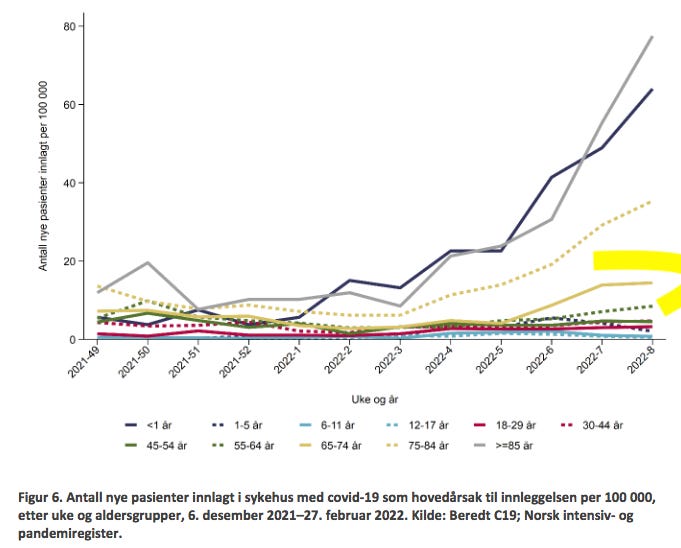
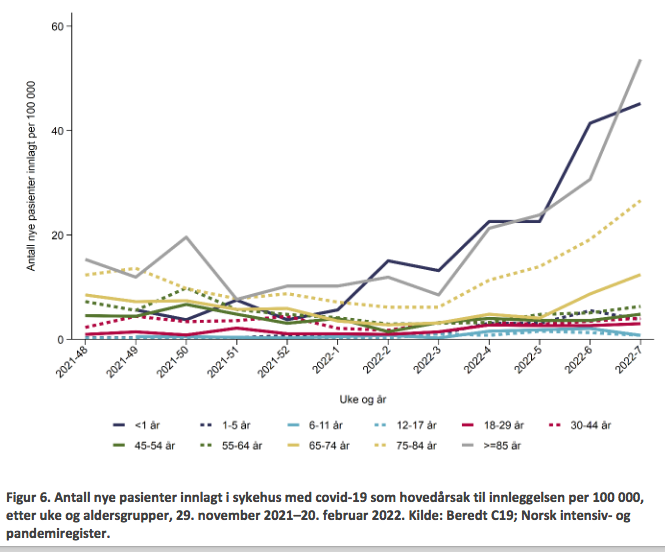
Note that this figure is similarly incorrect and misleading. In the summary, we noted that all the incidence rates for week 7 were corrected upwards, which you’d expect to see here. Astonishingly, nothing like that is visible here, and I’d say this is particularly galling with respect to the light brown-ish line (65-74yo) whose numerical rates increased, but here’s it’s flat. Do note the dotted green line (55-64yo), which appears to be turning upwards, much in line with the above numerical rate increase. For comparison, below is the same figure 6 from week 7 (p. 10):
Hospitalisation and Death Rates vs. Injection Status (pp. 13-14)
As mentioned last week, we’re at the ‘alignment’ stage now, by which is meant the ± same rates of hospitalisations of ‘all-cause vaccinated’ vs. ‘unvaccinated’, has been officially arrived at. 73% of the entire population has received at least two injections, which is mirrored perfectly by the 73% of hospitalisations (of those whose injection status was known), arrived at by adding 86 (2 doses) + 268 (3 doses), to which we must further add 13 ‘partially vaccinated’ individuals (1 dose, but didn’t—for whatever reason—take the second injection) + 2 (1 dose > 21 days before admission). Note that ‘alignment’ is temporary, as my expectation is that the share of esp. ‘boosted’ (3 doses) will continue to rise.
Like last week, the IPH, however, hedges its bets here, too, by adding that (p. 13):
In the past weeks, the share of hospital admissions of patients who received three doses has been rising, which is in part in line with the similarly rising share of the population who received three doses.
On the next page we get some perspective this week, which provides information ‘since the beginning of the vaccination program’ on 28 Dec. 2020. This information is summarised in Table 6 (p. 14):
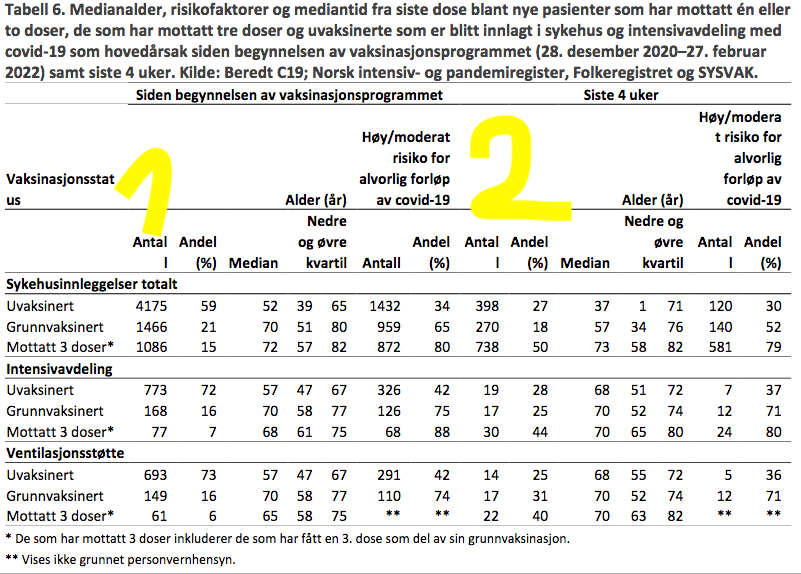
A few comments: note the totals since 28 Dec. 2020 (left-most column w/Numbers, indicated by the yellow ‘1’), which are quite high and rising still, so we would like to know how these changed over time, won’t we?
For comparison, we turn to data from week 39 of last year (27 Sept.-6 Oct. 2021)—why week 39, you may ask? Well, it’s the first time the share of hospitalisations of ‘vaccinated’ (back then: 2 doses) exceeded that of ‘unvaccinated’—to gain invaluable perspective on the rate of increase.
In the IPH’s report from week 39 (p. 11), we’ll find the following numbers: 193 ‘fully vaccinated and 70 partially vaccinated’ who were hospitalized since the beginning of the injection campaign. The median age of the ‘fully vaccinated’ (2 doses) was 77 years, and 148 (77%) were among medium-to-high risk groups for a severe course of Covid-19. Among the ‘partially vaccinated’, the median age was 52.5 year and 28 (40%) of them belonged to groups with elevated risk. Among the ‘fully vaccinated’, 24 (12%) required ICU admission, among the ‘partially vaccinated’, 8 (11%) required so. By comparison, of the 2,732 ‘unvaccinated’ admissions, 486 (12%) required ICU admission. All data relates to the time period elapsed since week 53 2020.
So, how did these groups fare since week 39? Here’s the breakdown:
Hospitalisations among ‘unvaccinated’: 2,732 (by week 39 2021) vs. 4,175 (by week 8 2022) = +53% in the 21 weeks since 6 Oct. 2021
Hospitalisations among ‘fully vaccinated’ (2 doses): 193 (by week 39 2021) vs. 1,466 (by week 8 2022) = +760% in the 21 weeks since 6 Oct. 2021
‘Booster’ injections became available on 5 May 2021, according to the IPH, but their numbers among hospitalisations weren’t disclosed by the IPH before week 48 (29 Nov.-5 Dec. 2021). Back in week 48, hospital admissions befell 55 ‘boosted’ (3 doses), 747 ‘fully vaccinated’ (2 doses), 106 ‘partially vaccinated’ (1 dose), and 3,022 ‘unvaccinated’ since 28 Dec. 2020. This allows us to calculate the increase of hospitalisations among ‘boosted’ individuals at least since week 48 2020:
Hospitalisations among ‘booster recipients’ (3 doses): 55 (by week 48 2021) vs. 1,086 (by week 8 2022) = +1,975% in the 12 weeks since 6 Dec. 2021
If this isn’t an unmitigated disaster, I don’t know what is—but I might offer a second aspect to this: ICU admissions during the time periods outlined below:
ICU admission among ‘unvaccinated’: 486 (by week 39 2021) vs. 773 (by week 8 2022) = +59% in the 21 weeks since 6 Oct. 2021
ICU admission among ‘fully vaccinated’ (2 doses): 24 (by week 39 2021) vs. 168 (by week 8 2022) = +700% in the 21 weeks since 6 Oct. 2021
ICU admission among ‘booster recipients’ (3 doses): 32 (by week 52 2021) vs. 77 (by week 8 2022) = +141% in the 8 weeks since 3 Jan. 2022
Sidenote: there are no ICU admission data of booster recipients before week 52 (27 Dec. 2021-2 Jan. 2022), which can be found on p. 13.
So, what can we infer from these data? I think the following observations are in order:
If there was ‘some protection’ offered by the currently available Covid-19 injections, the data shows its massive deterioration: two injections don’t protect against hospitalisation or ICU admission. Numbers for both categories have increased by +700% and +760% since 6 Oct. 2021 to-date.
The data is even (!) worse for ‘booster recipients’, at least when it comes to hospitalisation, which exploded by +1,975% in the twelve weeks (3 months) since 6 Dec. 2021.
There appears to be a somewhat larger (i.e., for now longer-lasting) protective effect with respect to ICU admission, or severe course of Covid-19, for ICU admissions among ‘booster recipients’ only rose by +141% in the past eight weeks since 3 Jan. 2022 (no data publicly available earlier). Note that, in fairness, these numbers will in all likelihood get progressively worse from here onwards as the IPH has told us the following last week:
During the last four weeks, the median time elapsed between the last injection and hospitalisation was 190 days (min. 150, max. 266 days) for those who received two injections, but it was 84.5 days (63-113) for those who received a third injection.
Note that ICU admissions among booster recipients are up 141% within the 90-120 days ‘worth’ of (some) protection afforded by the third injection. It’s reasonable to assume that these numbers will deteriorate from now on.
Now let’s move on to the ‘last 4 weeks’ (siste 4 uker), indicated by the yellow ‘2’ in the above table.
Hospitalisations (sykehusinnleggelser): ‘all-cause injected’ = 1,008 vs. 398 ‘unvaccinated’, which means the pace is quickening as that there are 153% more hospitalisations among the ‘all-cause injected’ (it was 106% last week).
Median age (median, the yellow shape between the two arrows): among ‘normal’ hospital admissions, the median age was 37 years (‘unvaccinated’) vs. 57 (2 doses) vs. 73 (3 doses); among ICU admissions, the differences are almost negligible by now (68 vs. 70 vs. 70); among those requiring mechanical ventilation, we see a comparable pattern (68 vs. 70 vs. 70).
There’s no need to change last week’s assessment:
It is fair to assume that the ‘normal’ hospitalisations among the ‘unvaccinated’ will be more like, well, maybe a one-night stay is required, and upon release there’s some prescription drugs to pick up (they are in the early 30s), which is very different from the ‘boosted’ admissions who were in their 70s. The same age ‘benefit’ may also be assumed to play out, albeit to lesser degrees, among the ICU admissions and those on a ventilator.
The share of medium-to-high risk patients (the right-most column) shows the numbers and shares of high-risk admissions among the ‘unvaccinated’ at about a thirty percent (‘normal’ hospitalisation, up from 27% in week 7). The share of ‘unvaccinated’ requiring ICU admission or mechanical ventilation rose a bit as well, for they are 37% and 36% (up from 23% and 22% in week 7, respectively), which is still considerably lower than two weeks ago (it was 50% in both categories in week 6).
Look again at the ‘injected’ (2 doses), though, for their shares didn’t budge and they are at 52% in week 8 (54% in week 7) among ‘normal’ admissions, and two times 71% among ICU admission and mechanical ventilation requirements (these stood at 75% and 71% respectively, in week 7), so essentially no change here.
Among ‘booster recipients’, there’s now a telling admission by the IPH: 80% of ICU admissions belong to medium-to-high-risk groups; last week, the IPH didn’t tell us about this, hence it’s fair to assume that if the IPH uses to askterisks (**), as it does with the mechanical ventilation requirements, it’s 80+ percent. Hence, these shares may have fallen a little bit, but they are still very, very high, esp. if one wishes to ‘sell’ the injections as preventing a severe course of Covid-19.
Here’s the visualisation, courtesy of the IPH (fig. 7, p. 15):

Compared to the last report, the risk of hospitalisation and ICU admission appears to be receding somewhat. In the past four weeks (weeks 5-8 2022), if you received 2 or 3 injections, your…
…risk of hospitalisation was 153% higher than if you remained ‘unvaccianted’
…risk of ICU admission 40% higher compared to an ‘unvaccinated’
…risk of requiring mechanical ventilation 36% higher compared to an ‘unvaccinated’
In other words, if one elected to forego these injections, one’s overall risk of serious harm from Sars-Cov-2 and Covid-19 is now considerably lower, much in line with data from the UK as reported by Igor Chudov.
Sidenote: Igor is doing a fantastic job of dissecting UK data, but we cannot compare these data sets without a few problems as the UK data focuses quite a bit on test positivity and data on reported positive tests, which the Norwegian data won’t allow us to do. We can compare the Covid-associated death rates, though, which we shall now do.
Last Words: Covid-associated Deaths
From the inception of the injection program through week 8 (2022), we know the injection status of 1,223 deceased (out of a total of 1,659 Covid-associated individuals). Of these 1,223 deceased, 582 (47.6%) were ‘unvaccinated’ (compared to 566, or 49%, as per week 7) vs. 603 (49.3%) affected those who either received two or three doses (of these 603, 175 or 14.3%) had received a booster injection (compared to 556, or 48%, as per week 7; similarly, the number of booster recipients stood at 136, or 12%, last week). To these numbers we may add 38 (3.1%) who passed away after 1 dose (29, or 3%, as per week 7). All data on this is found on pp. 18-19.
All told, since last week 6 (see here), the majority of Covid-associated deaths occurred among ‘all-cause injected’.
As always, here’s Table 8 (p. 19) with the current state:

Note that ‘all-cause injected’ continue to die at 3X the rate of the ‘unvaccinated’.
Brief Comment
I still don’t understand why people still take these injections. My first guess would be that there’s perhaps only a very small number of Norwegians who actually bother to check out these reports. Personally, I don’t think the IPH is disclosing everything they know about this, which will come back to haunt public services in a myriad of ways: once it will become widely known that the injections don’t work (anymore) and are actually quite harmful, someone will be left holding this particular bag.
I thus maintain last week’s comment:
It’s a stupid combination of ‘sunk costs’ (i.e., political and other capital invested is so high that one cannot step back without ruining one’s career) coupled with institutional inertia and the inevitable time-lag between the recognition of a problem, it’s acknowledgement, and eventual resolution. We’re not near the ‘recognition’ phase yet.
If the time-lag between test positivity numbers vs. hospitalisations, ICU admissions, and the requirement of mechanical ventilation of 3-4 weeks will hold, we’re in for a rather unpleasant surprise within the next few weeks: I expect these rates for the ‘all-cause injected’ to continue to rise, followed by another uptick in the death rate. I thus maintain what I wrote last week:
The rate of Covid-associated deaths for ‘all-cause injected’ is already 3X the rate of ‘unvaccinated’. Now, look again at the rates for ICU admission and mechanical ventilation, which in the past 4 weeks stood at 4X and 5X, respectively. I suspect, then, that the death ratio between ‘unvaccinated’ vs. ‘all-cause injected’ will rise to these (or higher) rates before too long.
I’d only add that with the seasonal peak of Covid (Omicron) almost behind us in Scandinavia, I suspect authorities and ‘experts’ to struggle to explain this. My guess is that the most likely ‘explanation’ that we’ll be offered (fed) to be that this was all caused by the revocation of the mandates—even though it’s been the IPH themselves who called for an abrogation of the mandates in early February 2022 as they were deemed more harmful than useful.
So, is it too far into ‘tinfoil hat-wearing’ territory to suspect the following: perhaps ‘Western’ gov’ts and public health authorities last hope is the extension of the Russian military operation in Ukraine to keep these unpleasant tendencies—which I think are pretty much baked into the situation, and there’s not much, if anything, anyone can or will be able to do about them anyways—from bubbling up.
That said, here’s the problem for the technocratic elites: go and look up ‘Rasputsitsa’, which will slow down the Russian army once it gets warmer in the next weeks. The window of opportunity of obscuring the injection failure (and the harm they do) will close within the next couple of weeks.
What will we be served to distract the people in April?
We need to get away from covid mortality and instead focus on all-cause mortality and morbidity (e.g., myocarditis) where we compare absolute values for vaccinated with unvaccinated and with a historical mortality and morbidity average.
Why? Otherwise we may miss non-covid adverse events from vaccines.
But the criminal agencies just provide junk data! There are only two data we need:
1) All causes hospitalizations and deaths among uninjected and injected of the same group of people and at the same time and place. This data is almost impossible to get except in an RCT, but we do have that:
https://www.canadiancovidcarealliance.org/media-resources/the-pfizer-inoculations-for-covid-19-more-harm-than-good-2/
2) Hospitalizations and deaths of different causes among the injected and uninjected compared to previous years. Have heart fibrillation, clotting, cancers, neurological greatly increased and is it only in the jabbed? This data should be easy to collect and it is being collected. Here in Sweden, they (Socialstyrelsen) will release data for 2021 in December 2022, because no hurry with the most important data, so better bullshit about "cases", vague definitions of "died with covid" and counting people who just got their second jab as "unvaccinated".