


Covid in Norway: Injection Safety Edition, pt. 2: more data on (severe) AEs, AE incidence reporting per injection, and a primer into modelling cumulative injection risks
Citizen reports of AEs took off as injections rose by 114% in June-July 2021, and looking at injections 1, 2, and 3 reveals how much your risk increases with each shot

In yesterday’s post, we’ve explored whatever drug safety data is published by the Norwegian Medicines Agency (NMA). After a brief overview, we focused specifically on those age brackets (0-11yo and women of child-bearing age) whose prominence in the recent drug safety report is quite something: the Covid-19 injections aren’t widely available to these age groups (0-11), and the public health authorities’ information on pregnancy and nursing is…lacking, to say the least. I addition, we also looked at a recent (non-refereed) paper by Trogstad et al. that looked into the ‘increased occurrence of menstrual disturbances’ after the Covid-19 injections.
As regards the following, if not noted specifically, all page numbers refer to the NMA’s drug safety report, with added emphases mine (if not noted otherwise).
Bottom line in these issues: like Sars-Cov-2 and Covid-19, your individual risk of being harmed by these genetic injections by BioNTech/Pfizer and Moderna—Norway doesn’t use the J&J or AstraZeneca products since spring 2021—is highly stratified by age and sex, so much so, that the NMA’s report contains a set of tables (p. 4), which break down the data by gender (table 1) and age (table 2):

Severe AEs (p. 5-7)
The NMA has so far processed 5,386 reports of ‘severe’ AEs, or 19% of the total number of reports received. For institutional reasons, these severe AEs are prioritised by the agency, hence they are currently slightly over-represented.
If the administration of a Covid-19 injection led to any of the following characteristics, the NMA considers it a ‘severe’ AE (p. 5):
persistent significant impairment
life-threatening illness or death
caused fetal harm and/or congenital malformations
resulted in hospitalisation irrespective of length of stay
or is found to be on the European Medicines Agency’s list of important medical events (which is part of the EudraVigilance AE reporting system)
The above statement is augmented by the following (ibid.):
Hospitalisation is the most frequent inclusion criterion for classification of an AE as ‘serious’, and this applies to 49%* of the severe AE reports. Hospital admissions include both patients who are admitted for observation and recover quickly and patients with life-threatening symptoms and diseases which causes permanent damage.
* The NMA has previously made a mistake when calculating the proportion of severe AE that have resulted in hospitalisation. We have calculated the proportion in relation to the number of severity criteria stated in the reports, for a side effect AE report can meet several severity criteria, hence [the earlier calculation] was incorrect. [I suppose because it resulted in much larger numbers of AE, but that would look ‘bad’ in the media, I presume…] The purpose has always been to calculate the proportion of reports that have resulted in hospitalisation in relation to the total number of serious reports. The percentage has been corrected as of the report on side effects per 4 January 2022.
A Brief Comment on the ‘Corrected’ AE ratio
I looked, however briefly, into the bimonthly-issued reports from 14 Dec. 2021 (here) 4 Jan. 2022 (here), and a cursory look into the relevant sections on pp. 4-5 in both reports shows that the share of processed AE reports actually decreased: in mid-December, 54% of all received AE reports were noted as processed, whereas in early January, it was 51%.
At the same time, the raw numbers of reported AEs increased: there were 45,153 AE reports as of 14 Dec. 2021, of which 4,203 (17%) were classified as ‘severe’; by 4 Jan. 2022, there were 48,682 AE reports, of which 4,528 (18%) were classified as ‘severe’; for the sake of it, I also looked at the NMA’s report for 18 Jan. 2022, which counted 51,985 AE reports, of which 4,766 (18%) were classified as ‘severe’. You may take a look at these reports yourself, which can be found here.
In the NMA report dated 4 Jan. 2022 (here), there’s but a brief footnote on the correction, which reads (p. 5):
Updated 10 Jan. 2022: The NMA has previously made a mistake calculating the proportion of severe AE reports that have resulted in hospitalisation. We have calculated the proportion in relation to the number of severity criteria stated in the reports. Since a side effect message can meet several severity criteria, this share was incorrect.
The purpose has always been to calculate the proportion of reports that have resulted in hospitalisation in relation to the total number of serious reports. This has been corrected as of this report.
Weirdly enough, in their report dated 14 Dec. 2021 (here, p. 5), the share of ‘severe’ AE because of hospitalisation was 44%, whereas in the current report (p. 5), this share is given as 49%. In other words: the correction contributed to a higher share of ‘severe’ AE reports, if ‘only’ due to higher hospitalisation rates.
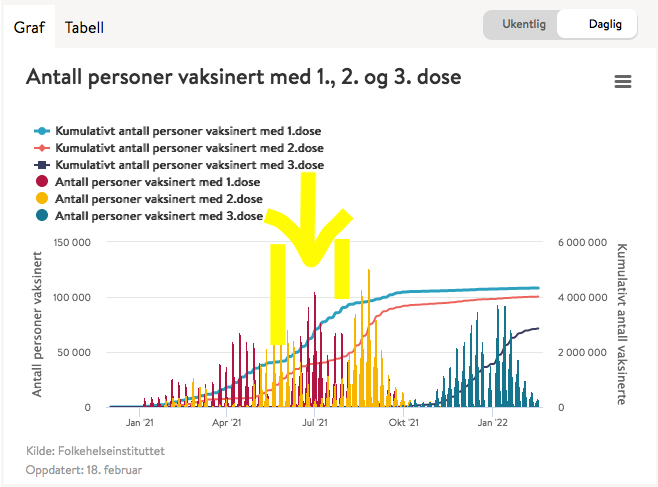
One more aspect to consider—and the below graph comes from the report dated 18 Jan. 2022 (here, the below visualisation is fig. 1 on p. 3)—is the question of who reports AEs to the NMA. The answer is—from July 2021 onwards, the overwhelming number of AE reports is filed by the affected residents (the orange line), as opposed to healthcare workers (HCW, helsepersonell in Norwegian, the blue line).

Sidenote: if you’re reading this and find yourself, sadly, in that ‘affected’ category, you can click here and file a report (if you haven’t done this already). Also, if you know someone who falls into this category, do pass along that information.
While the underlying data isn’t provided in the report, there’s—at least on my part—the suspicion that ‘something’ may have changed in late June and July 2021. Incidentally, the Institute of Public Health’s (IPH) bespoke website reveals that the cumulative number of first injections rose from 1,690,860 (1 June 2021) to 3,618,421 (31 July 2021) during precisely this period, a sudden jump by 114% during these two months, which helps—at least in part—explain the sudden changes to both the AE reporting incidence by the resident population. Note that the HCW-reported share didn’t suddenly increase, which suggests that more ‘regular’ people filed more reports. This can also be seen by simply looking at the graph provided by the IPH, specifically the area between the two horizontal yellow bars (there’s also an arrow to guide you), as well as the red lines, all of which is supportive of the above hypothesis that the rapid uptake of the first injections drove the increase in AE reports:
Back to the NMA’s Report
According to the NMA (whose listing is based on the respective EMA’s IME list), any of the following conditions are ‘severe’ (p. 6):
abdominal bleeding after menopause; loss of consciousness (syncope); pericarditis; blood clots in the lungs; myocarditis; deep vein thrombosis; anaphylactic shock; blood clot (thrombosis); arrhythmias (arrhythmia); blood clots or bleeding in the brain
These are listed according to their incidence, hence the most common (!) severe AE is quasi-menstrual bleeding after menopause, followed by passing out, etc. Note, further, that almost all of the other main categories are related either to blood coagulation (clots in the lungs, (deep vein) thrombosis, or bleeding/clotting in the brain) or cardiac symptoms (peri- and myocarditis, arrythmia).
(Reported) AE incidence of close temporal association with any of the injection products is summarised in table 3 (p. 7):

Note that * informs the reader that the category ‘total no. of AE reports’ is really the ‘number of AR reports that are processed’, i.e., these numbers will certainly go up; ** is the (dishonest, methinks) disclaimer stating that ‘even if someone dies in close temporal proximity to the administration of such an injection, it doesn’t follow that the injected product caused this death’; *** administration of the AstraZeneca product has been suspended in Norway on 11 March 2021, hence these numbers also incl. AE deriving from the AZ product administered abroad to Norwegian residents (who then filed an AE report in Norway).
There’s also a main comment to table 3, which reads:
It is impossible to directly compare the various Covid-19 injections as they are administered to individuals of differing age and comorbidity profile.
In my view, this is as close as it gets to admitting that all the ‘overall’ data—incidences of whatever, but esp. ‘safety and efficacy’ data—is very biased across age, comorbidity profiles, sex/gender, etc. Please remind me as to why we are insisting that everyone irrespective of these and other factors takes the same kind of product?
In yesterday’s post, I mentioned one of the major reporting-induced confounding variables:
Given the staggered nature of these injection, we’re not talking 11.2m injections administered to the same number of individuals; we’re talking about 11.2m injections spread out across 4.3m (1 dose), 4m of these same individuals (2 doses), and 1.9m ‘fully vaccinated’ people who rolled up their sleeves a third time.
A Primer into Risk Modelling for mRNA Injections
Let’s take it into account and, for the sake of the argument of sketching a very tentative risk profile, entertain the notion that both mRNA products (BioNTech/Pfizer and Moderna) were administered equally over time, i.e., they were administered proportionally (they weren’t, but hear me out):
Now, for the following, the guiding hypothesis is that risks associated (deriving) from repeat injections with these products increases cumulatively with the number of injections.
Shall we see if the data bear this out?
Based on the above-mentioned overall injection uptake numbers, the ratio between injections 1 : 2 : 3 is 2.15 : 2 : 0.95; to make this a bit less messy to calculate (it’s a very rough’n’dirty calculation anyways), let’s assume a ratio of 2 : 2 : 1.
Now, let’s divide the ‘total no. of AR reports’ by 5 and multiply the results by 2 (for injections 1 and 2) to arrive at a reported AE incidence ratio per injection (AEIR/I).
Finally, to arrive at the theoretical AEIR/I for injection 3, we multiply again by 2, as these are all cumulative factors.
With the preliminaries settled, let’s look at the data for the BioNTech/Pfizer product:
Injection 1: 6,010 AE reports, which yields a theoretical overall AEIR/I of 0.17%; for severe AEs, the theoretical AEIR/I is 0.04%, both of which are lower than the average.
Injection 2: theoretically, the no. of AE reports would be the same, but note that the no. of injections was considerably lower, hence the theoretical over AEIR/I would be 0.2%; for severe AEs it would be 0.05%; since the AEIR is cumulative (i.e., risk of an AE increased with the number of injections), the theoretical cumulative AEIR/I for ‘fully vaccinated’ individuals irrespective of any of the above-confounding variables would be 0.37% overall and 0.09% for severe AEs.
Injection 3: 3,005 AE reports, the theoretical AEIR/I would be 0.14%, overall and 0.03% for severe AEs.
In other words—and if my ballpark numbers are kinda o.k.-ish, methodically speaking (please let me know in the comments below)—the cumulative risk for overall AEIR after three injections with the BioNTech/Pfizer product would be somewhere in the ballpark of 0.51% overall and around 0.12% for severe AEs. Note that both numbers are in excess of the overall average, and they neatly show that risks deriving from injection with these products increases with the number of injections.
Now, shall we see if the hypothesis also holds by looking at the Moderna product data:
Injection 1: 2,028 AE reports corresponds to an AEIR/I of 0.37% overall and 0.08% for severe AE.
Injection 2: AEIR/I of 0.19% overall and 0.004% for severe AEs, i.e., 0.56% overall for 2 injections and 0.084% for severe AEs.
Injection 3: AEIR/I of 0.15% overall and 0.03% for severe AEs.
In other words, the cumulative risk for overall AEIR after three injections with the Moderna product would be somewhere in the ballpark of 0.71% overall and around 0.87% for severe AEs.
Brief Notes (Disclaimer) on these Risk Rates
Note that these ratios must be taken with a veritable salt mine, for they are nothing but mathematical playthings, even though they represent a somewhat o.k.-ish shot at making sense of the data available. I, for one, would love to have ‘better’ data, such as the inclusion of sex, age, comorbidity profiles, number of injections, etc. and the time periods these injections were administered.
Sadly, none of these data are published, hence my (puny) efforts to ameliorate the situation. Also, note that the AstraZeneca product seems to be particularly harmful, for it was ‘only’ administered in Norway from 27 Nov. 2020 through 11 March 2021, i.e., for 3.5 months, but it racked up an overall AEIR of 6.3% and 0.5% for severe AEs during this brief period along. By contrast, the J&J product came in with 0.5% overall and 0.05% for severe AEs, respectively, which is quite perfectly aligned with the overall AEIRs I computed. In other words: the AZ product is comparatively super-toxic and authorities have taken it off the table rightly so (and I’m shuddering to even ponder the AEIR/I for the AZ product after doses 2 and 3…).
That’s it for now, stay tuned for pt. 3 in due course.
Please let me know what you make of my amateur-ish risk ratio calculations.
The case you consider regarding cumulative AEIR/I is the case of equal chance of AE for each jab. Indeed, 15,024 AEs for 8,768,355 injections is an overall AER of 0.171%, and the cumulative AEIR/I (probability of suffering at least one AE) after three injections would be 1 - (1 - 0.171%)^3 = 0.513%. Probability of suffering two or more AEs is negligible.
However, consider the two hypothetical cases at the extremes:
- Case 1: AEs only happen with the first jab (if you're through that, you're fine). In this case, the cumulative AEIR/I for three jabs is equal to 15,024 / 3,616,466 = 0.415%
- Case 2: AEs only happen with the third jab (the first two are just saline solution). In this case, the cumulative AEIR/I for three jabs is equal to 15,024 / 2,185,632 = 0.687%.
Another interesting possibility: the first jab determines if you're an AE case, and you either get no AE at all (no matter the number of jabs), or an AE for each jab. AEIR/I for three jabs is then 0.171% - but it means buy one, get two free.
Interesting news from Germany (WELT article is behind paywall; haven't read it: https://www.welt.de/politik/deutschland/plus237106177/Coronavirus-Mehr-Impf-Nebenwirkungen-als-bisher-bekannt.html): health insurance providers have analyzed their data, which seem to indicate much higher AE rates (around 2.0%; the PEI official figures are at around 0.3%).
https://twitter.com/argonerd/status/1496571782094110721/photo/1