
Covid in Norway: week 7--injection failure: boosted at 3X risk of hospitalisation, fully vaxxed at 4X risk of ICU admission, 5X risk of ventilation required
all relative to 'the unvaccinated'; meanwhile, in the past 4 weeks, 'all-cause injected' die at 3X the rate of 'the unvaxxed'--with the above risks (even) higher, guess where the death ratio is going…

My reporting on the evolving Covid situation was kinda derailed this week by the Ukrainian emergency coupled with the National Medicines Agency’s latest report on the safety and efficacy of esp. the mRNA injections; needless to say, I also did some digging around the issue, which led to the three-part series (pt. 1, pt. 2, and pt. 3) and a number of notes on possible fourth injections, female reproductive issues, and severe adverse events.
While I have one more piece on these issues in the pipeline, today we shall return to the Institute of Public Health’s (IPH) update for week 7 (14-20 Feb. 2022). As always, I’ll provide you with the page numbers of sub-chapters and quotes, with all emphases mine.
One more word of warning before we begin: I’m unsure as to why these are, you know, explicitly labelled as Covid-related updates, for now the presentation has become so convoluted that one needs to read the phrases a few times to ‘get it’.
Executive Summary (pp. 3-4)
Hospitalisations for Covid-19 as main cause are up, rose to 399 in week 7 (up from 313 in week 6), which corresponds to a 27% increase week-over-week. Interestingly, the report also cites the overall number of new admissions in week 7, which stood at 764, of which hospitalisation for Covid-19 was given as main cause in 52% of the cases.
This week, we also learn a bit about the age profile, as ‘the number of new admissions per 100,000 inhabitants was highest in the age group of 85+’. Well, given the clear risk stratification, this isn’t a surprise, but what surprise me was the following breakdown of these rates by age group, incidence, and (some) numbers:
85+: incidence/100,000 = 53.6, n = 63
75-84: incidence/100,000 = 26.6, n = 82
65-74: incidence/100,000 = 12.4, n = 67
All other age cohorts had a hospitalisation incidence ‘of below 10 per 100,000’.
There was one outlier, though, and it fit into the space between 75-84 and the 85+ bracket, which is new-born children below age 1, which had an incidence/100,000 of 45.2 (n = 24), that means that 45% of children under 18 in week 7 were >1yo (70 of 156), which is (reasonably) explained by the ‘lower threshold for infant admission’. Further context is provided by the fact that ‘admission [of infants] is generally short-lived’ and the fact that ‘admissions due to Covid-19 in the age group <18 years is still significantly lower than what was registered for RS virus infections’ last autumn.
Of the 399 new admissions, the injection status was known in 329 cases. Of these, 87 (26%) were ‘unvaccinated’, 58 (18%) had received ‘basic immunisation with a maximum of two doses’, and 175 (53%) were ‘vaccinated with three doses’. While this development is certainly nothing that couldn’t be expected given the relationship between cause and effect, here’s how the IPH tries to spin this:
Vaccinated patients had an overall higher median age and a high proportion [of them] has conditions amplifying their risk [har risikofaktorer] that lead to increased risk for a severe course of Covid-19 relative to the unvaccinated.
Plain English: vaccine failure, expressed in so many words, for this is nothing but a rather carefully worded statement that the final sales pitch—that while not 100% effective, the injections would at least provide (some) individual protection from severe disease—has become untenable.
There are two more bullet points in the executive summary about ICU admissions and deaths, but there are ‘only’ numbers without context, hence and I shall say something about them further below.
As regards the test positivity, the Omicron wave appears to have crested in mid-February, but it might also be that the changes to the testing regimen in combination with the revocation of most mandates has contributed to this reduction. In other words: it might be a data artefact.
Final points here—injection uptake: as of 20 Feb. 2022, 73% of the entire resident population has received at least two doses; in the 16+ bracket, the share is 87%, and in the 18+ bracket, it is 89%. Of the entire resident population, 52% has received a booster injection, even though this breaks down differently across the various age brackets, with 89% booster uptake among 65+, 81% for those over 45, and 65% for those over 18.
Among high-risk groups aged 18-64, injection uptake stood at 80%, among those in the same age bracket with moderate risk, it stood at 72%.
Brief comments: I do appreciate the relative candour of the IPH when it comes to admitting ‘vaccine’ failure; yet, with injection uptake as high as it is now, there’s something strange about this—why now? I mean, it’s not as if these issues haven’t been ‘out there’ for some time (and not ‘just’ in my substack). My best guess would be that this is part and parcel of a hedging strategy to avoid a not-too-distant-in-the-future backlash over the failed public health policy masquerading as the Covid-19 injection program.
Why would I say that this is a more or less carefully worded fallback strategy? Well, here’s what I wrote on 31 Dec. 2021:
My expectation is that the trend lines [of un/injected hospitalisations] will cross once again in or around mid-January once the recently-boosted move past the 90-120 day expiration date of whatever protection is afforded by a third jab
And here is what I wrote about these trends in mid-January:
The gap between admissions of ‘jabbed’ vs. ‘unvaxxed’ patients is rapidly closing… it’s entirely reasonable to expect the ‘boosted’ category to overtake the ‘fully vaccinated’ category before the former will also overtake the ‘unvaccinated’.
While I take no comfort in having been right about this, what does the current report say?
First, some perspectives, courtesy of fig. 4 (p. 10), which plots the test-certified number of positive ‘cases’ (blue line) vs. the number of hospitalisations for Covid-19 as main cause (red line).
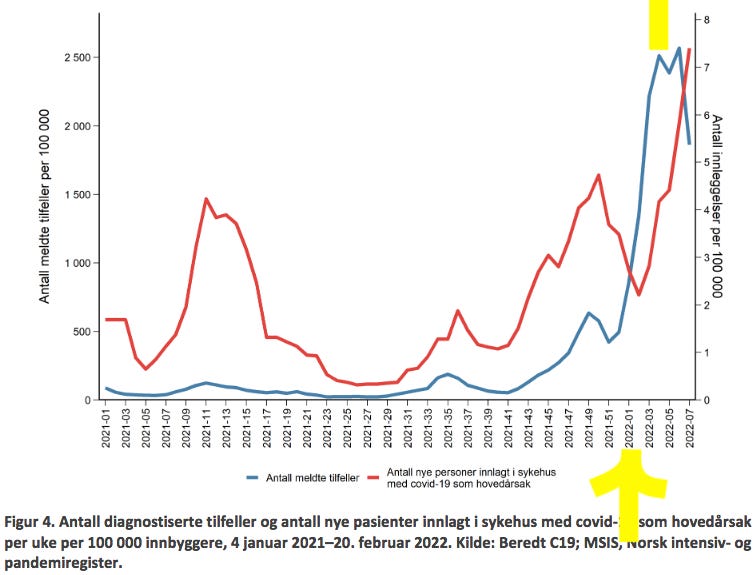
As indicated by the two yellow markers (bottom = week 1, top = week 3-4), hospitalisations lag positive tests by about ± 3 weeks, hence while the peak of the ‘testing wave’ may have arrived by now, it’s entirely predictable that hospitalisation will increase even more before that wave breaks. Note, further, that never before have hospitalisations for Covid-19 been higher in Norway.
Another way to show the problem of ‘Covid-19’ or ‘indirect Covid’ (the injections) contributing to a rather grim winter-and-spring season 2021/22 are the rising incidences for the 65+ age brackets, as shown below in Fig. 6 (p. 11).

Notice, in particular, how the dotted yellow-ish line (75-84yo) is about to shoot about like the grey trend line (85+), but don’t lose track of the light brown-ish line (65-74yo) looks like it’s doing the same, albeit each of these three brackets appears to be doing so with a 2-4 week-long time-lag.
You know, even though SYSVAK, the Norwegian electronic immunisation registry, presents the data in a very unhelpful way, we can clearly infer a correlation between booster injection uptake of these three age brackets during the last quarter of 2021:

It’s even more telling in the way OWID presents the same data:
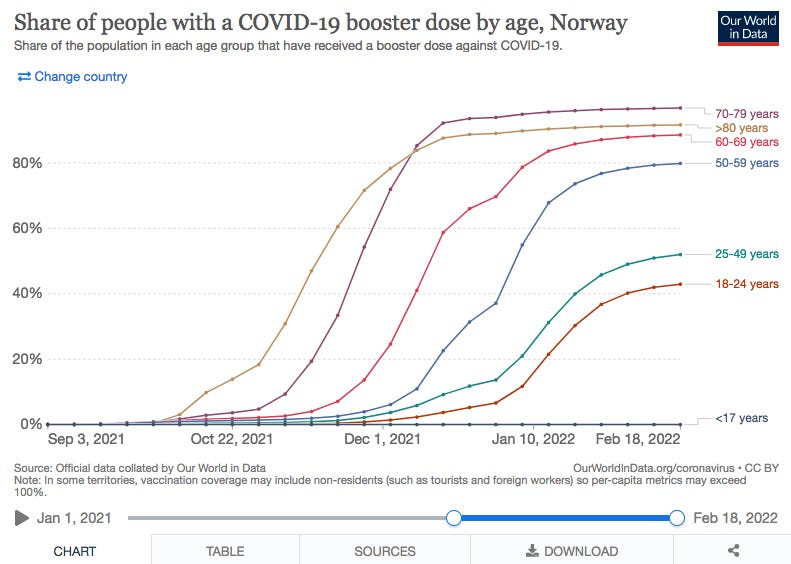
Bottom line: this is what happens 90-120+ days after the booster roll-out among these 65+ age brackets. Note that hospitalisation dynamics during the next couple of weeks will be driven primarily by the 75-84yo, 65-74yo, and, given booster uptake among the 50-59yo, also that age bracket, albeit to a lower degree due to the (so far) lower booster uptake.
Hospitalisation and Death Rates vs. Injection Status
As mentioned above, ‘alignment’, by which is meant the ± same rates of hospitalisations of ‘all-cause vaccinated’ vs. ‘unvaccinated’, has been officially arrived at. 73% of the entire population has received at least two injections, which is mirrored perfectly by the 72% of hospitalisations (of those whose injection status was known), arrived by adding 58 patients (2 doses) + 175 (3 doses) + 2 (1 dose). The IPH, however, hedges its bets here, too, by adding that (p. 12):
In the past weeks, the share of hospital admissions of patients who received three doses has been rising, which is in part in line with the similarly rising share of the population who received three doses.
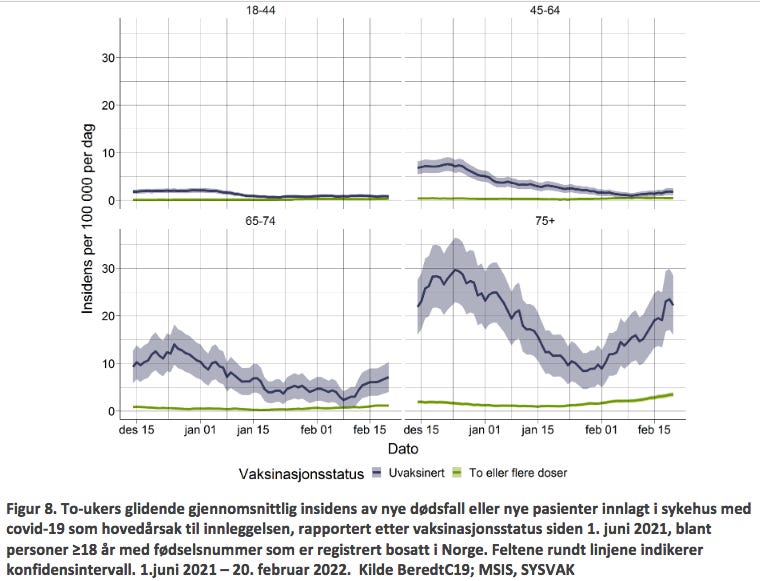
Interestingly, the IPH also points to the ‘calculated incidence rates per 100,000 inhabitants’ of both hospitalisations with Covid-19 as main cause and Covid-associated deaths, claiming that ‘since June 2021, and across all age brackets, these incidences were considerably higher for the unvaccinated’. Yet, a few lines further down, in the same paragraph, the IPH engages in regrettable obfuscation by stating (p. 12):
We have calculated the incidence in fig. [8 and 9 (p. 15)] in light of the daily numbers per injection category. Figure 8 shows the incidences for unvaccinated vs. those received two or three doses.
The figure itself is basically meaningless, for the IPH has mixed these important categories. Two injections after more than half a year mean basically no ‘protection’ whatsoever, and it’s completely beyond me why this category is folded into the same category as those who received three injections. It doesn’t make any sense, but it (still) gets worse, for the same paragraph continues as follows:
The incidence is clearly lower in the groups that have received three doses among those over 65 years of age. For the groups under 65 years, there is not much difference in incidence between two and three doses, probably since those with two doses already have a lower risk of a serious course.
This statement is clearly at odds with the numbers presented in the executive summary above, which show that the numbers of ‘all-cause injected’ (1, 2, or 3 doses) has been higher than those for the ‘unvaccinated’ for weeks. This entire paragraph doesn’t make any sense, and it doesn’t tell us anything—other than there’s either something wrong with the calculations (that’s clearly possible, for the Norwegian numbers—much like those from, say, Iceland must be mathematically adjusted to show incidence rates per 100,000, for the simple reason that the data base is too small due to the small population sizes) or these absurdities are indicative of a more problematic problem, by which is meant that this is a political statement, as opposed one based on data.
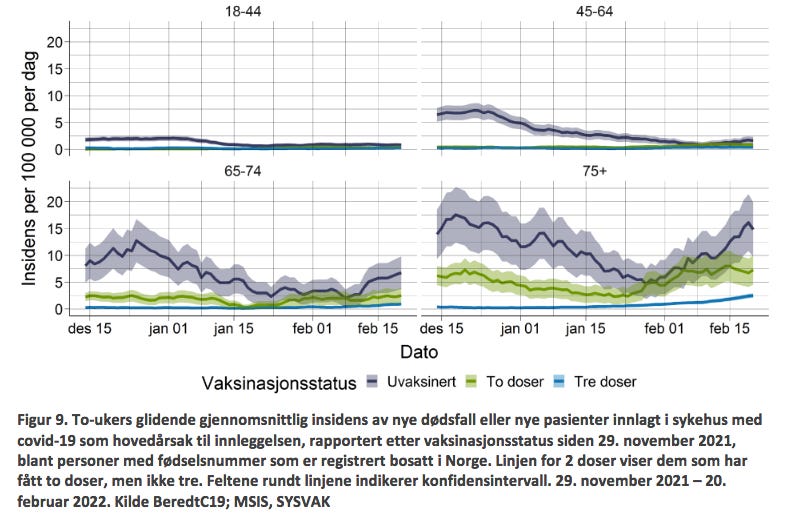
Without much further ado, here’s Figs. 8 and 9 (p. 15), but keep in mind that—again, and for whatever reason—the IPH uses 14-day moving average for both hospitalisations (fig. 8) and deaths per 100,000 (fig. 9). Here’s a bonus question for those among you with good eyesight: can you spot a meaningful difference between ‘unvaccinated’ vs. ‘all-cause injected’ under age 64?
Hospitalisation and Injection Status
Since the injections were rolled out (28 Dec. 2021), we are informed on p. 13, there were a total of 173 patients with 1 dose, 1,348 patients with 2 doses, and 702 patients with 3 doses, which means the combined total of ‘all-cause injected’ hospitalisations currently stands at 2,223 admissions. By contrast, there were 3,981 ‘unvaccinated’ patients admitted during the same period. We further learn that
Among those who are ‘basis-immunised’ [grunnvaksinert, i.e., 2 doses], the median age is now lower than before during the injection campaign. This reflects the high uptake of the third injection among the older age brackets. The share of those who are considered at medium or high-risk for severe disease is highest among those who received a third injection.
What is more, and perhaps this is the IPH’s way of telling us about abject ‘vaccine failure’, the text continues explaining that
During the last four weeks, the median time elapsed between the last injection and hospitalisation was 190 days (min. 150, max. 266 days) for those who received two injections, but it was 84.5 days (63-113) for those who received a third injection.
In other words: much like Omicron’s incubation period is about half that of the earlier variants, the third dose has similarly halved the time period (in days) between injection and hospitalisation. While this might be a weird coincidence, it’s certainly quite telling that the oft-proposed 90-120 days of protection offered by the ‘booster’ appears to be slanted towards the lower number of days.
Be that as it may, here’s the customary table 6 (p. 13), and do pay particular attention to the highlighted columns on the past 4 weeks (siste 4 uker) on the right-hand side.

As the numbers are already quite telling in and of themselves, I shall limit my commentary to the following few points (for comparison to last week, see here):
Hospitalisations (sykehusinnleggelser): ‘all-cause injected’ = 687 vs. 302 ‘unvaccinated’, which means that having received 2-3 injections carries an overall excess risk of 127% of requiring hospitalisation for Covid-19 compared to the ‘unvaccinated’. Note, further, that the hospitalisation rate of ‘all-cause injected’ stood at 106%, i.e., whatever protection the booster injection offered diminished by twenty (!) percent in the past week.
Median age (median, the yellow shape between the two arrows): among ‘normal’ hospital admissions, the median age was 33 years (‘unvaccinated’) vs. 51 (2 doses) vs. 73 (3 doses); among ICU admissions, the differences are almost negligible by now (65 vs. 60 vs. 69); among those requiring mechanical ventilation, we see a comparable pattern (65 vs. 65 vs. 67). There’s no need to change last week’s assessment:
It is fair to assume that the ‘normal’ hospitalisations among the ‘unvaccinated’ will be more like, well, maybe a one-night stay is required, and upon release there’s some prescription drugs to pick up (they are in the early 30s), which is very different from the ‘boosted’ admissions who were in their 70s. The same age ‘benefit’ may also be assumed to play out, albeit to lesser degrees, among the ICU admissions and those on a ventilator.
The share of medium-to-high risk patients (the right-most yellow arrow) shows the numbers and shares of high-risk admissions among the ‘unvaccinated’ at about a quarter (‘normal’ hospitalisation). In marked contrast to last week, though, the share of ‘unvaccinated’ requiring ICU admission or mechanical ventilation more than halved (it’s 23% and 22% now, respectively, down from 50% in both categories last week).
The share of ICU patients and/or those requiring mechanical ventilation, by contrast, among doubly injected has risen and now stands at 75% and 71%, respectively (up from 69% in both categories last week).
Risk Ratios for Hospitalisation, ICU Admission, Ventilation
What I find even more telling are the absolute numbers, which allow us to calculate risk ratios:
Hospitalisations: 83 ‘unvaccinated’ vs. 127 who received two doses = +53% higher risk of requiring hospitalisation for Covid-19 vs. 365 with three doses = +339% higher risk relative to the ‘unvaccinated’.
ICU admissions 3 ‘unvaccinated’ vs. 12 who received two doses = 4X higher risk; no data for those with three doses is given (I think the risk is even higher).
Mechanical ventilation: 2 ‘unvaccinated’ vs. 10 who received two doses = 5X higher risk; no data for those with three doses is given (I think the risk is even higher).
From what I understand from Igor Chudov’s recent piece on infection rates in the UK and the US, it’s apparently worse for Norway (I shall ask Igor).
Here’s the visualisation, courtesy of the IPH (fig. 7, p. 14):

Last Words: Covid-associated Deaths
From the inception of the injection program through week 7 (2022), we know the injection status of 1,160 deceased (out of a total of 1,596 Covid-associated individuals). Of these 1,160 deceased, 566 (49%) were ‘unvaccinated’ vs. 556 (48%) who either received two or three doses (of these 556, 136 or 12% had received a booster injection), to which we may add 29 (3%) who passed away after one injection (pp. 18-19). All told, since last week (noted here), the majority of Covid-associated deaths occurred among ‘all-cause injected’.
As always, here’s Table 8 (p. 19) with the current state:

Note that ‘all-cause injected’ continue to die at 3X the rate of the ‘unvaccinated’.
Brief Comment
Given these numbers and trendlines, I cannot explain why public health authorities still offer these products to the people. I wish I knew the answer, but at this point I may only venture a guess: it’s a stupid combination of ‘sunk costs’ (i.e., political and other capital invested is so high that one cannot step back without ruining one’s career) coupled with institutional inertia and the inevitable time-lag between the recognition of a problem, it’s acknowledgement, and eventual resolution. We’re not near the ‘recognition’ phase yet.
Speaking of time-lag, here’s another item of concern: if hospitalisations, ICU admissions, and the requirement of mechanical ventilation are occurring at these insanely high rates now, guess what this will do to death rates (‘unvaccinated’ vs. ‘all-cause injected’) within the next few weeks? I suppose you guessed correctly—they will go up (before they may or may not come down). The rate of Covid-associated deaths for ‘all-cause injected’ is already 3X the rate of ‘unvaccinated’. Now, look again at the rates for ICU admission and mechanical ventilation, which in the past 4 weeks stood at 4X and 5X, respectively. I suspect, then, that the death ratio between ‘unvaccinated’ vs. ‘all-cause injected’ will rise to these (or higher) rates before too long.
Finally, and this relates to the current mess in Ukraine (noted by me and the Naked Emperor, too), might the military escalation between Kiev and Moscow mark the moment where governments and their poodles in legacy media seek to ‘move on’ in the hope that no-one will bring up these unfortunate, if very clear, trends in polite conversation? It might well be, but it’s speculation. Still, I’d bet that this thought may have crossed a few minds.
Time will tell, any which ways.
Something to note, perhaps: Norway, as has Sweden, has school holidays during weeks 7-11. Different regions have holiday one week at the time so as not to overload the ski resorts and roads and such.
So week 7 was the first such week with people mingling at after-ski, living in small lodges, and so on. Meaning that after week 11 a great many families will have mingled and travelled hither and yon across the country - and then going back to school. As I know from personal experience, the week after sportlov (sport holiday) is always a week where you have lots of students and colleagues at home sick, and you can't find temps for money or mercy.
Don't b surprised if we get a Covid-bump between weeks 12-14. If the russian-ukrainian situation has moved on to at least armistice by then, we'll probably get more fear porn in the media as various political besserwissers will want to capitalise on it.
I love your article! I wish I could read the underlying PDF file.