


Covid in Norway, which will end (most) mandates soon, a new risk assessment by the IPH, and the current state-of-play: is Omicron really 'mild'?
2022 saw much higher rates of hospitalisation, ICU admission, and deaths, with esp. the latter accruing to 93% (!) in the elderly (60+). Join me as we explore the newest data released (pt. 1)

Apologies for the belated treatment, but as you know—there’s so much going on right now and the day has only 24 hours. Leaving aside these issues, let’s now focus on the past two weekly updates from the Norwegian Institute of Public Health (IPH) for weeks 4 (24-30 Jan. 2022) and 5 (31 Jan.-6 Feb. 2022); and because this post was somewhat delayed, I’ll also try my hand at an interpretation of the now available five weeks of Omicron data.
How are things in Norway?
A little background information before we dive into the data. Like its Nordic peers, esp. Denmark and Sweden, Norway has begun to re-emerge from its Covid-induced semi-lockdown a few weeks ago in mid-January. Since then, everyday life has returned to something like ‘normal’, although I’m unsure to call this a return to the ‘old normal’, as opposed to something else, which I don’t think is the full-blown ‘new normal’.
Schools, restaurants, hotels, and other amenities (gyms, museums, and the like) are open; in fact, schools were never closed down since spring 2020 (a big win for the kids), there were no mask mandates in primary and secondary schools, although the (esp. senior) high school students only started to return to their schools quite recently. Still, public trust in authorities, while not what it used to be, is still elevated relative to most other western countries, in particular as the visible effects of Covid-19 are at a quite low level.
Little systematic testing has been done (with precious few exceptions, no mass-testing of kids), and I brought up this particular difference with, say, Covidistan, in yesterday’s post: with only 5.25 tests per 1,000 inhabitants as of this week, Norway’s resident population ‘tested’ at 15.5X less than Covidistan’s.
Norway to End Mandates
Yes, you read this correctly—there’s almost no systematic testing over here, and word has it that as the authorities prepare to leave the fear-induced and panic-ridden phase of Covid-19-the-social-construct behind, the testing that is available will also change. Most notably, plans are currently discussed in media (e.g., here) to further reduce the incidence and availability of testing. What should be done, according to ‘many physicians’, is to ‘stop the unnecessary testing of asymptomatic people’, as per the Bergens Tidende, quoting the chief medical official of Norway’s second-largest city, Marit Voltersvik. What is more, all pertinent mandates from quarantine, self-isolation, and the like are similarly to be scrapped, according to Voltersvik (my emphases):
We see no longer any point in [mass-] testing, which should turn [revert] into something we do to determine clinical indication, by which is meant testing should be restricted to symptomatic patients.
and we are seeking to end all mandates and quarantine obligations. I think that should have been done by now. If you’re ill, you should, of course, stay at home.
This is unambiguously good news, if you’d ask me, but there’s more. According to a recent piece in Aftenposten (Norway’s NYT equivalent), the director of the IPH, Camilla Stoltenberg, is calling on the government to ‘go to normal everyday life shortly’. While there exists some uncertainty about the final size of the winter wave, the situation has improved to such a degree that there are no public health risks that should preclude an end to mandates.
Why would Norway do that now? I’m glad you asked.
A New Risk Assessment by the IPH
There’s even a sourced link—as in: Aftenposten appears to have begun to rediscover what journalists do—to the most current risk assessment (here), updated just yesterday. This most recent document is actually way shorter than the last iterations and clocks in at 29 pages, incl. front matter, which also provides an indication about the waning threat level, as perceived by public health authorities (by comparison, its predecessor was twice that long, if you care to check it out see here, or go directly to my take on it). The IPH’s main points are:
It’s not over yet, and there’s the expectation that the ‘flattening of the epidemic curve’ will occur around the end of the month, i.e., after the winter break.
3-4m Norwegians will likely be infected, with ‘a few thousands’ requiring medical attention, and ‘a few hundred’ will be admitted to the ICU.
There’s nothing any of the mandates will be able to do against this, and ‘any mandate may only serve to minimally reduce the number of infections’. In plain English: the mandates don’t work.
Most pressure will be on ambulatory services, GPs, nursing and retirement communities, with some related consequences throughout the economy due to elevated levels of sick leave at the same time (this is true, anecdotally: in my daughter’s kindergarten there were reduced opening hours last week due to large numbers of staff being, well, sick, and all of them are jabbed up to the hilt, by the way).
As regards autumn/winter and next year, the IPH expects population-wide ‘basic immunity’ (I’m unsure what that means, I mean—I can read and interpret it, but I fear what is meant that they hope that jabs plus infection will turn out o.k.; the original term is grunnimmunitet) will provide ‘good protection’ for any possible new variant.
There’s also more (fear porn) on influenza, but the main feature is the ‘let’s go back to normal shortly’ recommendation (p. 5). While this is unambiguously good news, there’s also a quite big, fat fly in the ointment: whereas the IPH admits to the inescapable fact that hospitals weren’t overrun in the past couple of weeks, and whereas this means elevated pressure on ambulatory services and first providers, there is still (!) no mention of early treatment options.
In other words: we’re super-fortunate that Omicron isn’t like, say, Delta (or worse), for if that wouldn’t be the case, this would be a mass-casualty event. I’m not a medical professional, but this statement reeks of intentional malfeasance.
Sidenote: Covid-19 is a very treatable disease, esp. if treated early on or, perhaps even better, prophylactically (and no, by this isn’t meant with experimental gene therapeutics, such as the mRNA and DNA injections), and after two years, public health authorities (sic[k]) still refuse to do anything to actually serve, well, public health.
For evidence of this, please go and read what, e.g., Kristin Greve-Isdal, the head of nursing staff (!) at Haukeland University Hospital (!) in Bergen had to say about ‘what to do if you get sick with Omicron’ as little as two weeks ago, as reported (paywalled) by Bergens Tidende: if you’re infected, stay at home, don’t take much in terms of medication against influenza-like illnesses, stay hydrated, and hope for the best. If you need medical attention, call your GP or emergency services.
This is as close as it gets in terms of intentional malpractice and malfeasance, and I shall not rant about it here. Instead, here’s some evidence that tells you otherwise (but I’m unsure anyone working in health care in Norway is able to read, you know, English), such as the Fareed-Tyson protocol via official South Carolina senate testimony, lots of prevention and treatment protocols from the Front Line Covid-19 Critical Care Alliance (I-MASK+, MATH+, I-RECOVER), or Peter McCullough’s treatment protocol (via America’s Frontline Doctors).
Keep in mind that I’m not a physician, this isn’t medical advice, and that every illness needs to be treated individually.
My point is this—there are many treatment options, but the Norwegian authorities are mum about them. They explicitly tell the population about the ‘treat (yourself) at home’ part, but they are wrongfully silent on how to do so. If I’d be an MP, I’d ask the IPH, the Health Directorate, and the Health Minister under oath about that latter part, but I digress.
Still—and here I fully recommend Igor Chudov’s writings on the subject matter who’s been voicing concerns and asking very critical questions about the perceived (wished-for) ‘mildness’ of Omicron—if you look at the IPH’s assessment, it’s hard to avoid these questions.

As can be seen in Fig. 3 (p. 8), hospitalisations are still growing, but now—this is the light grey area—Covid-related admissions have been superseded by what the IPH calls ‘other causes’ (the blue area). Yes, there’s some levelling off, but I’m not convinced that the still-rising incidence of hospitalisations is something that we’d simply should shrug off.

Similarly, Fig. 6 (p. 9) shows no end-in-sight (yet) to Covid-19 and other respiratory infections (the two light and dark blue lines shooting up).
The first five weeks of 2022 had already seen 895 hospitalisations, of whom 113 required ICU care, and 158 Covid-associated deaths, according to date presented in Table 1 (p. 9). Given the expected 3-4m of infections until the end of the month, that appears ‘mild’—but is it?
For comparisons, we turn to the IPH’s weekly reports from a year earlier, which show the following data.
Week 1: 89 (90) hospitalisations, 23 (22) ICU admissions, 37 Covid-associated deaths.
Week 2: 86 (91) hospitalisations, 14 (16) ICU admissions, 32 deaths.
Week 3: 78 (89) hospitalisations, 7 (11) ICU admissions, 19 deaths.
Week 4: 41 (47) hospitalisations, 9 ICU admissions, 21 deaths.
Week 5: 33 (34) hospitalisations, 6 (8) ICU admissions, 10 deaths.
Before we get to the cumulative totals for weeks 1-5 (2021), please note that the numbers in parentheses are the corrected numbers from a week later, which I’m using for the below calculation (as opposed to the weekly numbers; this is true for both hospitalisations and ICU admissions. For Covid-associated deaths, I’ve used data from week 6.
Hospitalisations: 351 (weeks 1-5 2021) vs. 895 (same period 2022)
ICU admissions: 66 vs. 113
Deaths: 119 vs. 158
This means that in weeks 1-5 2022, hospitalisations are up by 155% relative to the same period a year earlier, ICU admissions by 80%, and Covid-associated deaths by 33%.
If we now turn to Table 1 (p. 9), we are able to calculate, however imperfectly, a tentative case rates, or incidences, for these three categories.

Now, let’s have a look at Fig. 7 (p. 17), which breaks down these numbers by age cohort (confusingly, not by the same age brackets as Table 1, but, hey, you work with the data you’ve got, not with the data you’d wish you had).
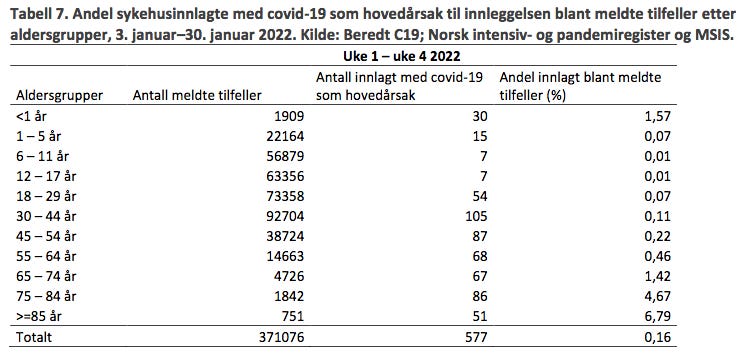
The most notable things to mention are the incredibly high rates in all three categories we’ve looked at so far among those aged 60 and older. All below numbers etc. are from Fig. 1, i.e., they cover the period 1 Jan. through 6 Feb. 2022, and the contrast to the much smaller shares of these age brackets as shown in Table 1.
93% of all Covid-associated deaths occurred among 60+ residents.
53% of all Covid-associated ICU admissions occurred among 60+ residents.
And 42% of all Covid-associated hospitalisations among 60+ residents.
Note that this current (9 Feb. 2022) assessment is devoid of any detailed information with regard to ‘vaccination uptake’. This is particularly obvious if compared to the more detailed listing on pp. 13-14 in the last assessment (26 Jan. 2022), which held that among 65+ residents, uptake was 91% (which means it’s certainly higher now).
Sidenote: do not ask me why the IPH doesn’t use the same age brackets consistently, for I don’t know, but I don’t think it’s ill intent (stupidity typically suffices). I think that this is due to someone setting up certain tables one way, which were later augmented and/or reformatted, hence the unhelpful discrepancy.
So, to sum up this part—if we assumed a 1 : 1 mirroring of ‘vaccine uptake’ among the 60+ cohorts (which, for practical purposes we shall assume to be equal to 90%), Covid-19-the-disease has turned into a ‘pandemic of the elderly’ (doh, it always was).
Still, the main question that arises at this point is: the above back-of-the-envelope assumption is certainly not much more than a quip, and we shall explore its implications in tomorrow’s post.
I think the difference in severity of Omicron is due to differences in the health of the sampled population. Scandinavia is far and away from the pandemic of morbid obesity, heavy smoking and lack of exercise that is typical of the populations that have been hit harder than us.
That observation holds true when looking inside our nations here too: diabetes, hypertoni, being fat, having a generally unhealthy lifestyle wthout exercise or proper food and vitamin D deficiency: 80%+ of those dead from/with Covid had one or more severe comorbidities.
This is of course unscientific in that I have zero studies to show. On the other hand I would hazard a guess that the number of studies who individually looks at the things listed above number in the tens of thousands, as regards to general health.
And as a personal self-aggrandizing anecdote: I'm semi-retired. I am in better health and physical condition than the average 18 year old. The volunteers I meet at church (all of them 70+ save one) are all spry and healthy because they grew up being physically active to an extent which is virtually onknown for city-dwelling children born post 1980 at the latest.
It all adds up, I think. But how to measure it, well - that's too complicated for me.
I am still undecided about the severity of Omicron. Is some countries it looks worse but in the UK, unless they are fiddling with the stats, it does look more mild.