


The Ghost of Covid Injections Past
In a stunning reversal, Norwegian public health officialdom now speaks of 'immunity' vs. Covid-19 without once talking about 'vaccines' (because there's no data to do so)

When I first saw the below-reproduced piece, I was unable to believe my eyes: did Norway’s arch-vaxxer Preben Aavitsland—he who never disliked any injectable concoction because Science™—and director of epidemiology at the Norwegian Institute of Public Health really say what he said?
Well, turns out he did, and because this might be of interest beyond Norway, I’ll give you state broadcaster NRK’s most recent absurdity masquerading as ‘journalism™’ (of course, it was written by their journo of choice, Jan-Erik Wilthil, yes, he who has a track record of writing about many matters related to ‘Covid’ but failing, as always, to ask the right questions).
Hence, while I hope you’ll appreciate the below content (in my translation, with emphases and [snark] added), be aware of the enormous amounts of gaslighting employed by both Aavitsland and Wilthil.
IPH: We are Expecting a Corona Wave in Late Winter
By Jan-Erik Wilthil, NRK, 3 Jan. 2025 [source]
For the first time in five years, Norwegians were able to celebrate Christmas without the company of a Corona wave. This is due to increased immunity in the population, according to the IPH [Institute of Public Health].
Since the start of the pandemic, the [sic] coronavirus has caused regular waves of infection around the world. So far, the virus has caused major outbreaks of infection when the cold weather sets in, but this year the expected winter wave has been a long time coming.
The situation has been the same throughout Europe, according to a report from the IPH [I’ve had a look at this piece, and I’ll have more to say about it below the translated NRK piece].
The long-lasting wave from last autumn still seems to be on its way down.
Thus Preben Aavitsland, acting director of epidemiology at the Norwegian Institute of Public Health.
This particular [autumn] wave may have saved many people from becoming bedridden over the Christmas period. In a report on the outlook for respiratory diseases this winter [same report linked above], the IPH points out that this outbreak made many Norwegians more immune to the virus variants now circulating [I’m unsure what part of the report Mr. Wilthil has read, but I can merely find one mentioning of ‘efficacy’, which reads as follows:
The recommended COVID-19 vaccines are expected to be effective against this [XEC] variant as there is limited immune escape from JN.1 or KP.2 mRNA booster vaccines [p. 10; note that there is no data underlying this statement]
There are, however, 27 mentions of variations of ‘immune–’, including this
It seems that the immunity from the summer wave is still adequate for this XEC variant and the new updated vaccine booster also helps against this variant [p. 10; note that this statement precedes the above; I’ll have more to say about the booster juice below; for now, note that natural immunity is what helps, as per the IPH—and now back to the article].
At the moment, there are the KP. 3.1.1 and XEC variants that dominate in Norway.
So far, no new variants have emerged anywhere in the world to cause concern, with Aavitsland adding:
The waves of COVID-19 will continue, but they will be less noticeable because the population’s basic immunity makes the infections generally milder. This means that a smaller proportion of those infected will experience severe COVID-19 disease, while a larger proportion will be infected without symptoms or with just a cold.
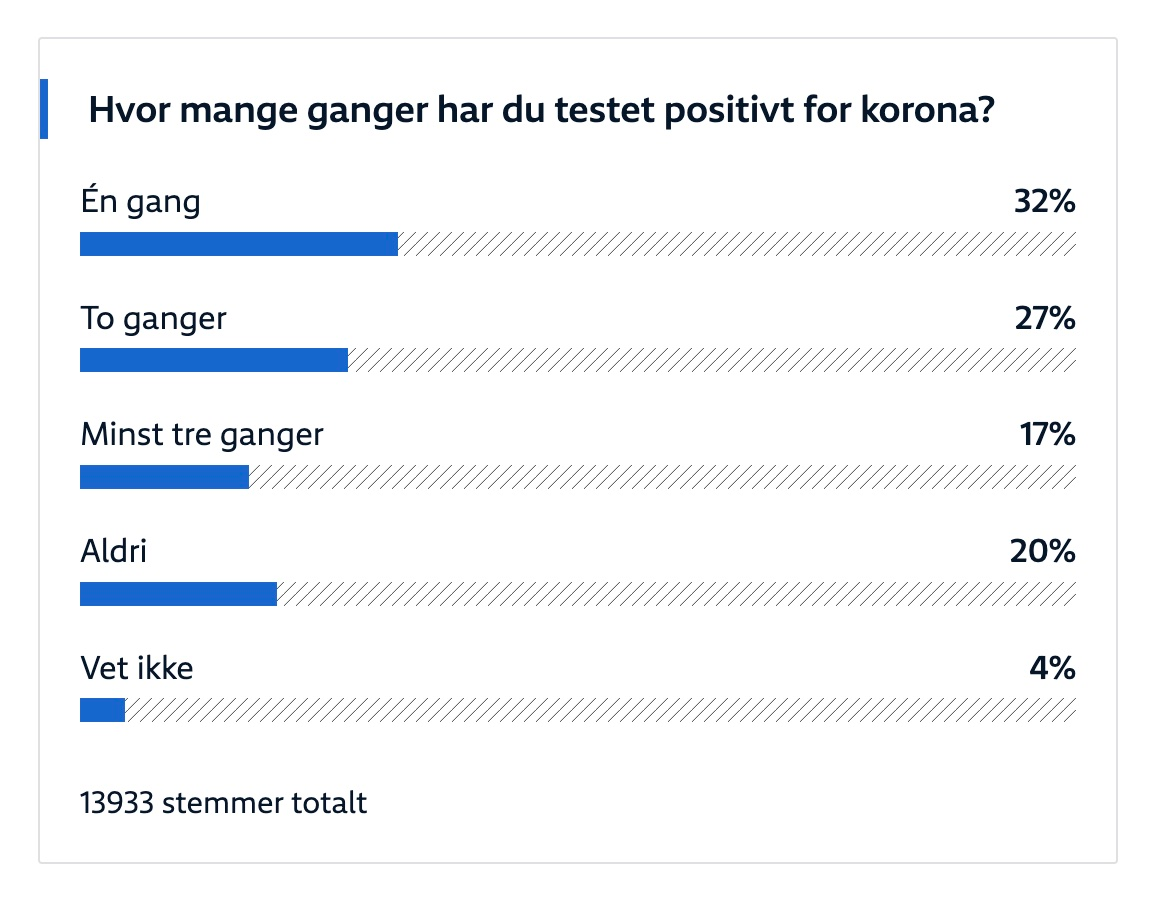
‘How often did you test positive for Covid?’—once: 32%; twice: 27%; at least thrice: 17%; never: 20%; don’t know: 4% [I didn’t participate; time stamp: 4 Jan. 2024 around 5:45 a.m. local time]
Expecting a New Wave of Infection
This does not mean that the danger is over. If a new and more potent virus variant emerges, corona could make a strong comeback.
‘We expect a new wave of COVID-19 in late winter,’ says Aavitsland [of course you do, who attention-seeking *****].
He points out that immunity to new infections weakens within a few months of the previous infection or vaccination [note that this is the only time ‘vaccines’ are mentioned; and then—take note that the above polling indicates that around a third of participants tested positive once/don’t know (care) which kinda puts the onus of proving his statement about vaccine efficacy on Aavitsland who, of course, doesn’t provide any evidence for his pro-vaxx statement (note that Mr. Wilthil, once again, fails to ask for data], or when the virus acquires new properties. This can lead to a resurgence of the virus.
‘New waves occur when a large enough proportion of the population is no longer immune to being infected’, says Aavitsland.
He believes that improved immunity is the most important explanation for the fact that waves of infection have decreased in both frequency and size.
[Wilthil] Is the disease becoming endemic?
[Aavitsland] SARS-CoV-2 is already endemic in the sense that it is always here, and will always be here. Population immunity prevents large waves, and the incidence is fairly predictable. It’s been clear since 2020 that this was the future for this virus.
[There are so many insults I’d like to hurl at Aavitsland and his ilk right now, incl. why the mandates/measures, incl. the demonisation of ‘import infections’? Take a look at Sweden’s choices, you moron; and if it’s been clear since 2020, why did—and, more so, why are you and your ilk still pushing the modRNA poison/death juices?]
Brief Comments on IPH’s ‘Outlook for the Respiratory Virus Season 2024/25’ and the Most Recent ‘Respiratory Virus Report’ (Week 50/2024)
First of all, I checked both reports (and not just the one linked by Mr. Wilthil).
Second, the ‘Outlook’ (p. 4) is crystal clear about Covid:
Covid-19 incidence is low. It is uncertain when the next COVID-19 outbreak will occur. As of now, there are no variants in circulation that indicate that the situation will change in the near future.
Immunity to influenza and SARS-CoV-2 in the population is generally good, but the elderly have very low protection against infection with newer SARS-CoV-2 variants and a booster vaccine is recommended.
And now we may ask ourselves as to why Dr. Preben ‘let’s jab everyone’ Aavitsland doesn’t say that when prompted by Mr. Wilthil. As a follow-up, we may also marvel whether the latter actually read the ‘outlook’.
T-cell immunity from vaccination and previous infection is also expected to limit the number of seriously ill…
The corona vaccines and infection have contributed to the fact that most people in Norway have now built up good immunity to covid-19 [p. 8]
Needless to say, no evidence for this assertion is cited, nor did Mr. Wilthil ask about it.
Does so-called hybrid immunity exist?
(This is a kind of excursus, skip if you wish to get to my bottom lines.)
Personally, although I’m not a physician, I don’t think so as there is no evidence for it, and I’ve compiled a laundry list of links, information, etc.:

The most relevant study I found (I asked Grok to help me with it, and its answers are, well, see for yourself) is by Fei Gao et al., bears the title ‘Spheromers reveal robust T cell responses to the Pfizer/BioNTech vaccine and attenuated peripheral CD8+ T cell responses post SARS-CoV-2 infection’, and it appeared in the journal Immunity, 56, vol. 4 (2023).
It looks legit, but it’s highly absurd (remember, this was transmitted to the journal in July 2022 and published in March 2023)—here is the summary:
T cells are a critical component of the response to SARS-CoV-2, but their kinetics after infection and vaccination are insufficiently understood [we’re talking summer 2022]. Using “spheromer” peptide-MHC multimer reagents, we analyzed healthy subjects receiving two doses of the Pfizer/BioNTech BNT162b2 vaccine. Vaccination resulted in robust spike-specific T cell responses for the dominant CD4+ (HLA-DRB1∗15:01/S191) and CD8+ (HLA-A∗02/S691) T cell epitopes. Antigen-specific CD4+ and CD8+ T cell responses were asynchronous, with the peak CD4+ T cell responses occurring 1 week post the second vaccination (boost), whereas CD8+ T cells peaked 2 weeks later [did the authors look for them after 2 weeks?]. These peripheral T cell responses were elevated compared with COVID-19 patients. We also found that previous SARS-CoV-2 infection resulted in decreased CD8+ T cell activation and expansion, suggesting that previous infection can influence the T cell response to vaccination.
Please re-read that last sentence once more, and then ask yourself: does this sound like ‘proof’ or even smell ‘convincing’?
Further down in the paper, there are the following insights:
We probed a total of 351 blood samples collected from vaccinated volunteers with time points ranging from pre-vaccination up to 4 months after the first dose [well, at least they looked longer than 2 weeks]…We observed lower frequencies of spike-specific T cells in circulation after infection compared with mRNA vaccination, especially in the CD8+ T cell compartment with a skewing of the response hierarchy among the tested epitopes. We also noticed qualitative differences in the virus-specific T cells. Vaccination led to the rapid induction of effector T cells that contracted by day 90, concomitant with an increase in the frequency of memory T cells. By contrast, only low levels of virus-specific memory CD8+ T cells could be detected in COVID-19 patients, even at 5 months post-symptom onset.
From the results section, we may learn the following:
Three independent cohorts: (1) SARS-CoV-2 naive individuals who received the BNT162b2 vaccine, (2) COVID-19 patients with SARS-CoV-2 infections, and (3) Individuals who received the BNT162b2 vaccine after recovery from a SARS-CoV-2 infection [looks legit, eh?]…
To study the development of anti-SARS-CoV-2 CD8+ T cell immunity mediated by vaccination versus natural infection, we compared the responses of SARS-CoV-2 naive vaccinees and COVID-19 patients…The patient cohort was established during the first wave of the pandemic (June–December 2020) and was most likely infected by the Wuhan-Hu-1 SARS-CoV-2 strain that matches the vaccine formulation [i.e., data comes from the trial population].
I’ll interrupt the flow here to indicate the following issue: doing so may have been relevant in spring/summer 2021 when considering any ‘booster’ jabs. Doing a study [sic] in 2022 with data from the wild type strain vs. the original modRNA poison/death juice is…pointless as the Wuhan strain was extinct by then.
We observed divergent spike-specific CD8+ T cell response after vaccination and infection in terms of the preferred epitopes…spike-specific CD8+ T cell response in circulation elicited by infection was lower in magnitude in comparison to vaccination…BNT162b2 vaccination induces a T cell response exclusively to spike peptides since the vaccine encodes only that protein. By contrast, SARS-CoV-2 infection generates a response against the whole virus…
We also measured the effect of BNT162b2 vaccination or SARS-CoV-2 infection on CD4+ T cells.
The true bombshell is tucked away further down in the piece, though:
We saw a marked difference in memory CD4+ T cells between the two cohorts [vaxxed vs. unvaccinated]…Analogous to the CD8+ T cell response, mRNA vaccination resulted in the rapid recruitment of spike-specific effector CD4+ T cells…By contrast, natural infection resulted in a more even distribution of spike-specific CD4+ T cells across the effector…these results suggest differences in how CD8+ and CD4+ T cell responses are triggered by SARS-CoV-2 infection versus BNT162b2 vaccination…
We also investigated the effect of mRNA vaccination in subjects who had previously recovered…response in these individuals…were 12.5-fold (at day 42) and 11.3-fold (at day 28) higher.
A bit further down, there is also this gem re hybrid immunity:
In another study evaluating protection conferred by mRNA vaccines and previous infection against Omicron in a prison cohort (a high-risk population), the authors observed higher levels of effectiveness from vaccination among staff in comparison to previous infection. However, no difference was observed in the inmates.49 However, it is important to note that these results are contrary to that observed by Altarawneh et al.50 They observed a higher effectiveness of previous infection (alone) against symptomatic BA.2 infection in comparison to two doses of BNT162b2 mRNA vaccine (>6 months before infection) in naive individuals.
This, by the way, is how the fake these studies: the one linked in footnote 49 (see here) compares ‘vaccination and previous infection against infection with the B.1.1.529 (omicron)’ in the California prison system while Altarawneh et al. (see here) is ‘national, matched, test-negative, case-control study in Qatar from December 23, 2021, through February 21, 2022’ that incl. both modRNA poison/death juices.
And that’s before the meaning sinks in: the above-related paper by Fei Gao et al. compares but the BioNTech/Pfizer concoction vs. the wild type in a small sample long after the Alpha variant had gone extinct, it’s—useless. (So much for ‘AI™’, which, by the way, originally pointed me to a Time magazine piece discussing the paper.)
Also, there doesn’t seem to be a good evidence-based case for hybrid immunity—yet Aavitsland still pushes this nonsense (as he did for some time now, and if you wish to read something really cringe-worthy, see this:)

Bottom Lines
I’ve only mentioned one of the reports (the ‘outlook’), and here’s the regular ‘status report’ (week 50/2024). While I’ll spare you most details, here is the main take-away:
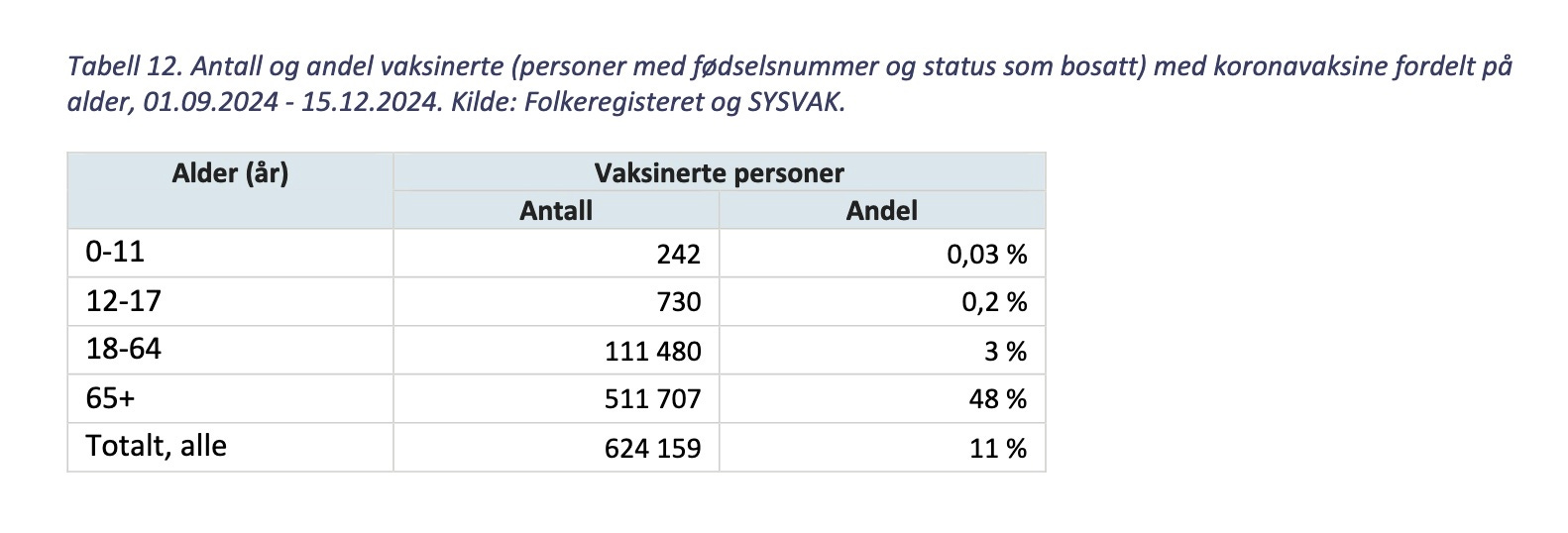
Table 12: number and share of vaccinees (persons with social security number and resident in Norway) vs. coronavirus broken down by age cohorts, 1 Sept. 2024-15 Dec. 2024.
You saw this correctly—the total shares of people under 65 taking booster jabs is slightly higher than 3%, with their ‘total, all of the above’ standing around 11% of the entire population indicating—that either that share of ‘vaccinees’ is good enough to have ‘good immunity’ (Aavitsland) or, which seems more likely to me, that the modRNA poison/death jab doesn’t do much, if anything, to prevent infection or transmission (pun intended).
From the ‘status report’ (p. 38), however, we may also learn the following:
The purpose of the corona vaccination programme is to prevent serious illness and death [hence the memory-holing of anything that reeks of transmission or infection]. The protection achieved, either through vaccination or illness, will diminish over time. This is primarily because the virus changes. It is therefore important that the target groups recommended for vaccination take a booster dose of the updated vaccine every year to ensure the best possible protection.
Most people have some protection against COVID-19 as a result of vaccination and/or illness. Vaccine efficacy (protection) after booster doses must therefore be calculated in relation to the protection of those who have not taken a booster dose [and this is how public health officialdom fakes its relevance: can’t they design a study that includes all these data points, incl. never jabbed, infected once and thereafter?]. Studies therefore calculate relative vaccine efficacy [i.e., models].
No efficacy data is yet available for this season, but a Danish study from 2023 shows that people aged 65 years and older had a 76% reduced risk of hospitalisation due to COVID-19 shortly after vaccination with the XBB.1.5 vaccine in the 2023/2024 season. However, a follow-up study showed that vaccine efficacy against the new variants BA.2.86, including JN.1. was slightly reduced, to 64% relative vaccine efficacy.
Here is the Danish study from last year, and I’d argue it’s useless as it studies the BA.2.86 subvariant, including 1615 JN.1 infections, which is irrelevant this year as they no longer exist.
Hence, from that paper, we ‘learn™’:
Severity analysis showed no evidence of association between the infecting variant and the risk of COVID-19 hospitalisation…no evidence of differences in self-reported symptoms by variant strain
Translation: we can’t tell the difference of outcomes.
I’ll leave you with this gem of ‘da Science™’:
[statistical] odds of infection with JN.1*, as opposed to a non-BA.2.86 variant, were 1·60 (1·27–2·02) times higher among XBB.1.5-vaccinated participants than among those who had not received this vaccine. Note that these results are not suggestive of an increased risk of infection with BA.2.86* or JN.1* among individuals who had received the XBB.1.5 updated COVID-19 vaccine, only that the vaccines work less well against these than against other variants.
Ouch.
I’m not even bothering with the preprint about antibody levels in Norwegian seniors in May 2024, because they only studied antibody levels, as opposed to memory cells (and thus found that antibody levels wane: ‘da Science™’ hard at-work; note that all seniors took 3-6 modRNA injections, median: 5).
What may we deduce?
Legacy media is continuing the gaslighting, and now they have been joined by public health officialdom.
No-one really wants to talk about why we continue to vaccinate against Covid-19, esp. as there appears little data and even less well-designed studies.
Speaking of ‘da Science™’, they are still doing relative vaccine effectiveness calculations (which is what Big Pharma originally did—remember the ‘almost 100% effective’ charades?), and I hold that they are doing this to obscure the piss-poor efficacy.
I’ll conclude with a gem from the ‘status report’ (p. 39):
The relative vaccine efficacy following a booster dose of the updated XBB.1.5 vaccine in autumn 2023 was estimated to be 50.6% shortly after vaccination [this merely means it’s a coin toss, at best] and was highest against XBB.1.5. Ten to 14 weeks after the booster dose, the relative vaccine efficacy had fallen to 42.2% [you’re ‘protected’, relatively speaking, for …*drum roll* ‘2-4 weeks’, as per Kirsebom et al.]. The effect was significantly lower against newer virus variants, including JN.1.
So, that paper shows coin toss-like levels of ‘protection™’ for ‘2-4 weeks, followed by waning to 13.6% (95% CI: -11.7 to 33.2%)’. Let that sink in.
Effectiveness was lower against both JN.1 and EG.5.1 variants with confidence intervals non-overlapping with the effectiveness of the XBB sub-lineages at 2-4 weeks for EG.5.1 where VE was 44.5% (95% CI: 20.2-61.4%) and at 5-9 weeks for JN.1 where VE was 26.4% (95%CI: -3.4 to 47.6%).
This is the best evidence (models) there appears to be speaking in favour (sic) of getting yet another jab.
And this is what the Institute of Public Health deduces from ‘da Science™’:
The results above show that those who take a booster dose of the updated vaccine are better protected against severe COVID-19 during the autumn and winter seasons than those who do not vaccinate even if the virus changes.
You can’t make this up. At least the people wisened up and, for the most part, stopped following these recommendations.
I personally think that next time around, though, if public health officialdom recommends another round of jabs, results won’t be different as there was no judicial review of what these ‘experts™’ did.
The same goes for ‘journos™’ who still don’t ask relevant questions and, apparently, don’t do their homework.
Shudder.
Fundamentally,anyone who talks about ‘Covid infections’ is talking nonsense because nothing was spreading. This has been conclusively demonstrated in analysis of the global excess mortality statistics by Denis Rancourt. Once you take on board this fact, the rest of the narrative, measures, vaccines etc all crumbles.
https://odysee.com/@shortXXvids:e/Rancourt-1---nothing-was-spreading:8
I wonder: Is Covid still that big a deal in Norway as it seems? Here, it's only ever brought up in the context of BP/AP (Before Pandemic/After Pandemic) as point of temporal reference to events.
It's like nothing happened, and we all agree on what it was didn't happen, kind of thing. Also, unsettling and eerie.