

Gardasil / HPV Agit-Prop in Nordic Media
Gardasil / HPV Agit-Prop in Nordic Media

Long-term readers might remember a long-ish piece about Merck’s HPV ‘Vaccine’ I penned last year. I detailed one tragic ‘sudden’ and ‘unexpected’ death of a young woman that occurred in close temporal proximity to the administration of the second dose of a HPV ‘vaccine’:


Starting in July 2024, Austria made available—for ‘free’—HVP injections for all people under 30, even though safety concerns have never been adequately addressed, much less discussed. Of course, the Health Ministry is pushing these jabs as hard as they can, and ignorance about injectable products once more reigns supreme.
What, then, inspired this posting? Well, this kind of agit-prop and drug pushing (pun intended) isn’t happening ‘just’ in Austria; it is happening literally everywhere in the West, including—Norway, of all places.
The below parts of this posting address, first, an article that went online just today at Norwegian state broadcaster NRK today; below, I shall provide a brief compilation (and commentary) on the HPV jabs deriving from official sources about the products mentioned in the article (because these insights are, of course, omitted from the media piece).
Non-English content comes to you in my translation; emphases mine.
Parents Give Their Children a More Expensive HPV vaccine: ‘I think you should have access to the best’
More parents are choosing to take their children out of the childhood vaccination programme to give them a better vaccine. Experts believe more people should have the opportunity.
By Viktoria L. Hellem-Hansen, NRK, 9 July 2024 [source]
‘I want my child to have the best possible cover with regard to HPV infection. That’s why I chose to do it’, says Per Bjørnstad from Hamar.
His son has received two doses in the childhood vaccination programme, which uses the Cervarix vaccine.
But like many other parents, the father of the family wants to take his child out of the programme so that he can buy the most expensive vaccine for his son:
I think you should have access to the best and the one that covers the most viruses.
Bjørnstad normally works for the Norwegian Cancer Society [orig. Kreftforeningen]. He says he is therefore well aware of why the vaccine is better than the one offered today.
According to experts, the Gardasil 9 vaccine covers far more viruses that can lead to cancer.
Björnstad adds: ‘It would have been nice if the information had been available to everyone, and not just to those who know about it, where this is talked about a lot.’
This is HPV and these are the Vaccines [this is from an info box]
The vaccine used in the Norwegian childhood vaccination programme is called Cervarix and only protects against HPV16 and HPV18.
Some HPV types can lead to genital warts. Cervarix does not protect against this, but Gardasil 9 protects against HPV types 6, 11, 16, 18, 31, 33, 45, 52 and 58.
In Norway, 7th grade girls have been offered the HPV vaccine since 2009. Boys since 2018. Both boys and girls in birth cohorts from 2006 and later have been offered Cervarix, which protects against HPV 16 and 18 [call this a mantra, or fetish]. So far, the focus has been on eradicating cervical cancer in Norway.
HPV is a common virus that is easily transmitted through sexual contact. Most people get one or more infections during their lifetime.
Condoms do not provide complete protection against HPV infection because the virus is also found on areas of skin in the genital area that condoms do not cover. Condoms are important to use to protect against other sexually transmitted diseases.
Most HPV infections go away on their own. [why take these jabs?]
There is no screening programme for HPV-related cancers other than cervical cancer [what’s the false positive rate for cancer screenings? Guess what, according to the literature, ‘false-positive cancer screening test results are common’, e.g., for mammography the rates are 50-61%: what could go wrong?]
Source: Helsenorge.no [this is the Norwegian healthcare insurance corp.]
More People are Dropping the Standard Vaccine
NRK has spoken to several parents who have taken their child out of the national vaccination programme and given Gardasil 9 to their children, but few want to come forward with this [in case you’re wondering why: because it’s supremely un-Scandinavian to do so, but, as with many other things up North, there’s a difference between ‘theory’ and ‘practice’]
Head of the health centre in Hamar, Ragnhild Elisabeth Eliassen, knows of ten cases where children have been taken out of the programme in her area:
Most people choose to follow the nationally recommended childhood vaccination programme [I’m sure I’m an outlier in this regard, because conformism in these things runs very high].
Eliassen says that there may be more cases they don’t know about [classic Nordic ‘splainin’: don’t ask, don’t tell, no problemo; I consider this piece a very limited hangout because here we’re talking about people doing something un-Nordic because they want ‘more’ jabs; we won’t need to hold our breath thinking about when media will discuss the case of parents opting out of these vaccination programs due to safety concerns after the Covid jabs].
Figures show that there is an increase in the purchase of the vaccine for children aged 10-14, which costs a total of NOK 5,000 for three doses:
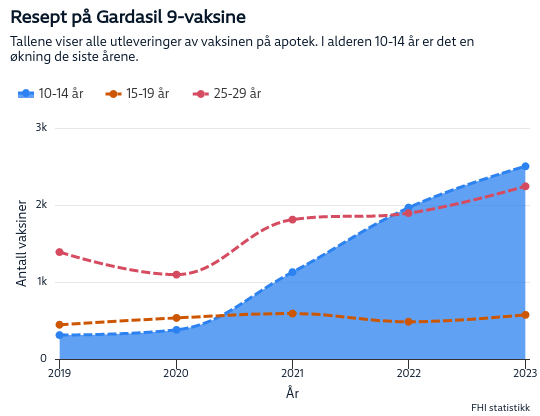
Prescriptions for Gardasil 9 vaccines: this chart shows dispensation of vaccines in drug stores; in the age bracket of 10-14yo, there was an increase in the last years.
People Don’t Want Differences
‘For many years, the professional community has been concerned about the use of Cervarix in the childhood vaccination programme’, says senior consultant Andreas Hopland.
He works in the Department of Cancer Surgery at Radiumhospitalet [the national cancer centre].
He and the national experts in the treatment of HPV diseases recently sent a letter urging a change in the choice of HPV vaccine in the childhood vaccination programme:
We are committed to ensuring that children are vaccinated in the best possible way and as broadly as possible against HPV disease caused by the HPV virus, including precancerous lesions, cancer and other types of disease.
The letter also states that they are concerned about socio-economic differences in Norway, because those who can afford to pay and know about the vaccine get the best protection [of course, there’s no discussion whether or not anyone should take these injections in the first place; it’s a faux debate about two such products].
This year there is a new round of vaccination offers, and the scientific community wants Gardasil 9 to be offered instead.
This means that two or more vaccine suppliers are competing for which HPV vaccine will be used as part of the childhood vaccination programme next year [apart from what ‘the Science™’ wants, Big Pharma wins].
Hallstein Husbyn, Head of Unit at the Norwegian Directorate for Medical Products, explains this in an email.
Getting a Vaccine that Doesn’t Cover Everything
Hopland believes that the Cervarix vaccine currently being administered is a good vaccine [remember that we just learned that ‘the professional community has been concerned about the use of Cervarix’, which contradicts Hopland’s ‘belief’ (sic)]. He says doctors are happy that it is being administered, adding:
But Gardasil 9 is a better vaccine, which also covers several HPV viruses that cause cancer, with direct protection.
He adds that the vaccine has been approved in the USA and will soon be approved in Europe as a vaccine against cancer of the oral cavity, i.e., ear, nose and throat cancer.
‘This is the HPV cancer that is increasing the most in Norway and Europe. There has been a fourfold increase. While penile cancer has also doubled.’
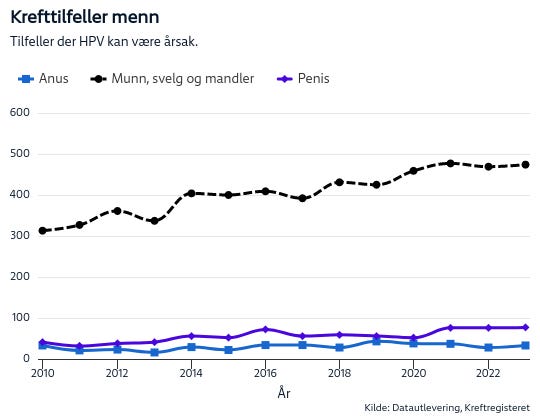
Incidence of cancer among men: cases in which HPV can be the reason. Anus = anal, or rectal; munn, svelg og mandler = mouth, throat, and tonsils.
For example, one of the HPV viruses covered by this vaccine, but not the current vaccine, can lead to RPP [Recurrent Respiratory Papillomatosis] and genital warts:
RRP is a disease that requires a lot of resources, especially for the children born with it, with a double-digit number of operations for them. It is a disease for which there is no treatment, but it can be prevented by immunisation.
Hopland herself receives referrals for the most difficult cases of genital warts, where they have to provide fairly extensive treatments and reconstructions of the patients’ genitals.
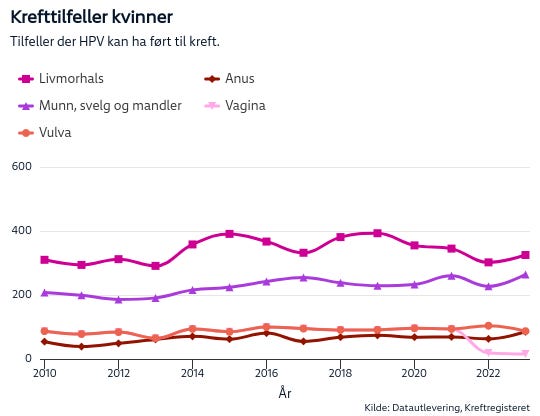
Cancer rates among women: cases in which HPV can be the reason.
Livmorhals = cervical cancer; Anus = anal, or rectal; munn, svelg og mandler = mouth, throat, and tonsils.
Hoping For a Political Decision
Hopland says that the scientific community wants politicians and decision-making authorities to know what they recommend and want for children.
Hopland hopes that there will be a political decision in favour of a vaccine that covers both genital warts and RRP more broadly:
In the long term, this could save society money as these diseases will not need treatment when they disappear [does the HPV jab actually work?]. It will also probably be possible to scale down the cervical cancer programme in the long term by providing broader HPV vaccine coverage.
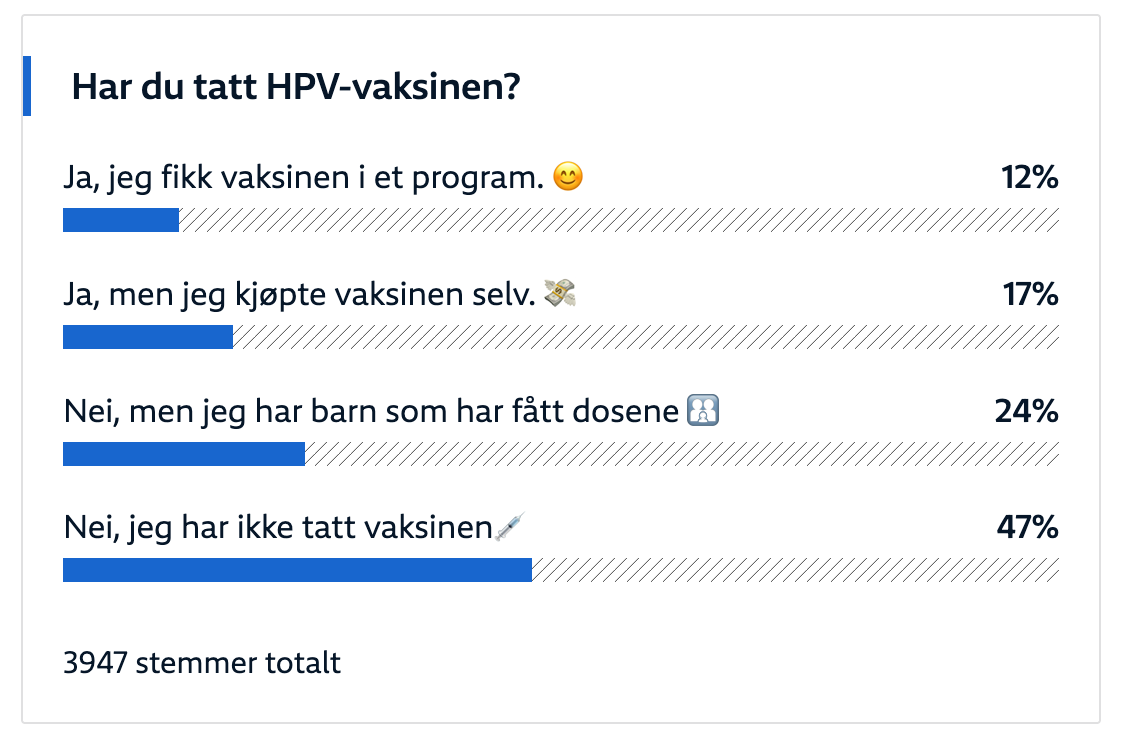
Did you take the [sic] HPV vaccine? Yes, via the national vaccination program (12%); yes, but I did it on my own (17%); no, but my kid(s) are vaccinated (24%); no, I didn’t take the [sic] vaccine (47%).
Bottom Lines
The above piece from NRK is literally how ‘the North™’ works: high levels of conformism coupled with strong steering from ‘the Experts™’. The above ‘debate™’ is about one kind of HPV vaccine (Cervarix) vs. another (Gardasil 9), which is to say: there’s a lot of stuff that’s simply not mentioned, such as the information about that young woman who died after her second dose of the HPV vaccine (linked in the posting above).
It is arguably worse, though, if you look at the wording provided by ‘the experts™’: these injectable products offer ‘protection’, yet their own (!!!) data doesn’t show a noticeable decline in cancer incidence.
What about the efficacy, then? Well, prescriptions for Gardasil 9 rose from 311 (2019) to 2,503 (2023), which is an eight-fold increase in five years. At the same time, the incidence of the cancers Gardasil 9 is said to protect people from also rose. How about that?
Here are links to available safety data (sic) websites, such as the CDC:
Findings from many vaccine safety monitoring systems and more than 160 studies have shown that HPV vaccines have a favorable safety profile—the body of scientific evidence overwhelmingly supports their safety.
By contrast, here’s what Gardasil 9’s package insert says:
Limitations of Use and Effectiveness
Vaccination with GARDASIL 9 does not eliminate the necessity for vaccine recipients to undergo screening for cervical, vulvar, vaginal, anal, oropharyngeal and other head and neck cancers as recommended by a health care provider [remember that the false-positivity rate in such screenings may be higher than 50-61%].
GARDASIL 9 has not been demonstrated to provide protection against disease caused by:
HPV types not covered by the vaccine [see Description (11)],
HPV types to which a person has previously been exposed through sexual activity [i.e., if you cannot be sure your intimate partner(s) are jabbed and tested on a regular basis, the jabs don’t work].
Not all vulvar, vaginal, anal, oropharyngeal and other head and neck cancers are caused by HPV, and GARDASIL 9 protects only against those vulvar, vaginal, anal, oropharyngeal and other head and neck cancers caused by HPV 16, 18, 31, 33, 45, 52, and 58.
GARDASIL 9 is not a treatment for external genital lesions; cervical, vulvar, vaginal, anal, oropharyngeal and other head and neck cancers; CIN; VIN; VaIN; or AIN.
Vaccination with GARDASIL 9 may not result in protection in all vaccine recipients [oh, how about that?]…
The safety of GARDASIL 9 was evaluated in seven clinical studies that included 15,703 individuals who received at least one dose of GARDASIL 9 and had safety follow-up. Study 1 and Study 3 also included 7,378 individuals who received at least one dose of GARDASIL as a control and had safety follow-up. The vaccines were administered on the day of enrollment and the subsequent doses administered approximately two and six months thereafter. Safety was evaluated using vaccination report card (VRC)-aided surveillance for 14 days after each injection of GARDASIL 9 or GARDASIL.
Translation: we compiled data for 14 days after administration of the last jab. That’s it.
Deaths in the Entire Study Population
Across the clinical studies, ten deaths occurred (five each in the GARDASIL 9 and GARDASIL groups); none were assessed as vaccine-related. Causes of death in the GARDASIL 9 group included one automobile accident, one suicide, one case of acute lymphocytic leukemia, one case of hypovolemic septic shock, and one unexplained sudden death 678 days following the last dose of GARDASIL 9. Causes of death in the GARDASIL control group included one automobile accident, one airplane crash, one cerebral hemorrhage, one gunshot wound, and one stomach adenocarcinoma.
Systemic Autoimmune Disorders
In all of the clinical trials with GARDASIL 9 subjects were evaluated for new medical conditions potentially indicative of a systemic autoimmune disorder. In total, 2.2% (351/15,703) of GARDASIL 9 recipients and 3.3% (240/7,378) of GARDASIL recipients reported new medical conditions potentially indicative of systemic autoimmune disorders, which were similar to rates reported following GARDASIL, AAHS control, or saline placebo in historical clinical trials
I wrote all of the above before Aaron Siri wrote his lengthy posting about the missing safety data for any vaccine. These issues are entirely absent from the above-related NRK piece. Trust ‘the Science™’, indeed.
Moreover—and a move that’s even more damning (as well as revealing)—there is plenty of ‘other’ information from very much ‘the Science™’ that should have been included in the above-related NRK piece, such as this piece from the National Cancer Institute from 2021:
Despite more than 15 years of consistent evidence that HPV vaccines are safe and effective, a new study has found that more parents are citing concerns about the vaccines’ safety in recent years. The findings highlight an urgent need for doctors and public health leaders to address these concerns with parents, according to the scientists who led the study [by means of…suggesting to parents to skip that crap?]…
Some parents have always cited concerns about safety for declining to get the HPV vaccine for their kids. But from 2015 to 2018, the study showed, the percentage of parents who declined the HPV vaccine for their kids due to safety concerns nearly doubled. During the same time frame, reports of serious health issues after HPV vaccination were consistently rare, the study found.
Results from the study were published September 17 in JAMA Network Open.
And then there’s the currently-ongoing Gardasil Trial against its manufacturer Merck, which, just earlier this spring, moved to the ‘discovery’ phase:
Our law firm is looking at various Gardasil lawsuits, focusing on premature ovarian failure and premature menopause claims and we talk about their potential settlement amounts and jury payouts and why we think the premature ovarian failure and menopause claims are likely the strongest cases both a trial and for settlement.
Many women to the HPV vaccine and later suffered from an unexpected disease. Now they want to know if the root cause of their problems was the Gardasil shot…
March 2024 Update
Earlier this year, Merck’s Gardasil defense team filed a motion with the MDL Judge to dismiss all of the Gardasil lawsuits, arguing that the failure-to-warn claims made by the plaintiffs are legally prohibited under the National Childhood Vaccine Injury Act. However, last week, MDL Judge Kenneth Bell issued a memorandum opinion partially denying the motion and allowing the litigation to move forward. Judge Bell ruled that claims alleging Merck’s negligent failure to inform healthcare providers about Gardasil’s potential risks are not entirely barred under the Vaccine Act, nor are claims of Merck’s fraudulent concealment of these risks. This decision holds significance as it paves the path for the progression of the Gardasil litigation into the subsequent phase, potentially prompting Merck to pursue a comprehensive settlement agreement.
May 2024 Update
Last week, Merck sought to dismiss a group of three Gardasil cases from the MDL, arguing that the plaintiffs in each case had failed to exhaust their administrative remedies under the National Vaccine Injury Act. This Act mandates that all plaintiffs in vaccine-related cases must first present their claims in vaccine court before proceeding to civil court.
June 2024 Update
Lawyers representing both sides in the Gardasil HPV vaccine multidistrict litigation (MDL) are nearing the end of the discovery phase for the initial set of bellwether test cases. The date for the first Gardasil bellwether trial is anticipated to be established at tomorrow’s MDL status conference. However, it appears probable that the first Gardasil test trial will take place in California state court. This California case involves a plaintiff who claims to have been left bedridden for life due to the Gardasil vaccine.
Buyer beware, parents inform yourselves.
All of the information in these bottom lines—and I’m certain there’s tons more—are omitted from the above piece. It’s a shame and a disgrace, and all I hope is that not more children get hurt by these products.
What a pity that girls have been offered the HPV vaccine since 2009, and the cancer diagram only starts in 2010... are pre-2010 data to be found anywhere?
Great article. Thank you. I also saw this one today. Gardasil Fails to Protect Against Cervical Intraepithelial Neoplasia Over Time https://petermcculloughmd.substack.com/p/gardasil-fails-to-protect-against?