


Upside-Down, Again: More from the EMA's 'Assessment Report' from Feb. 2021
More on the 'ostrich approach to public health decisions': no data has been asked for, no data has been collected anyways, and what is there is ludicrously under-powered

As we held in Saturday’s overly long posting on ALC-0315, there’s quite bit ‘more’ information in the EMA’s safety assessment (from January 2021) for the BioNTech/Pfizer product. This post today continues Saturday’s post and highlights some of the more egregious issues with EU Commissioner Kyriakides’ reference to it in February 2022.
If you care to remember, we left the EMA’s assessment in the section on repeat dose toxicity, and we shall continue to go through that report. As a brief reminder, here’s how this particular section concludes (p. 52, my emphases, as elsewhere below):
In conclusion of the preclinical pharmacology, the presented data, including immunogenicity, triggering of neutralizing antibodies and Th1 response and reduced presence of viral RNA in challenged animals as well as radiological lung parameters, provide support for the vaccination approach. Due to species differences in the immune system between animal model species and humans, the conclusion whether this candidate vaccine will be sufficiently effective in humans needs to be established in clinical studies.
Now, Commissioner Kyriakides, why on earth would you respond (on 9 Feb. 2022) to MEP Reil’s question about safety and efficacy of ALC-0315 and ALC-0159 in such a condescending manner as if the above-quoted assessment by the EMA would be conclusive in this regard?
Here’s Ms. Kyriakides:
The quality of the ALC-0159 used as an excipient in Comirnaty has been demonstrated to be appropriate for its intended use and is in compliance with the relevant EMA scientific guidelines and standards expected for all medicines.
No mention of ALC-0159, as I’ve held, but it’s about the quality of the product, not its potential effects (which is what MEP Reil asked about). It suffices to know that ALC-0159, similarly manufactured by Echelon Biosciences Inc., is also ‘for research use only’, according to the product information, reproduced below:

Next up, On Pharmacokinetics and Toxicity of Comirnaty (pp. 53-56)
The two novel lipid excipients play different roles in the formulation and have different pharmacokinetics. It is worth to notice that the lipid displaying a persistent kinetic over time in liver is ALC-0315…
ALC-0315 is an ionizable aminolipid in BNT162b2 and is the most important lipid component for efficient self-assembly and encapsulation of the mRNA within the LNP, and for providing successful delivery of mRNA into target cells.
The PEG-lipid (ALC-0159) is designed to largely exchange out of the LNP after administration and before uptake into target cells, whereas the aminolipid (ALC-0315) is critical to the efficient intracellular delivery of the mRNA through endosomal uptake and release and must remain with the LNP.
Further down in the EMA document, there are the following passages, even though I’m kinda dying to learn what is, really, meant by ‘self-assembly and encapsulation of the mRNA within the LNP’.
The Applicant pointed out that during the course of the 2-week pharmacokinetic study, liver concentrations of ALC-0315 fell 4-fold from their maximum value indicating that 75% of the material delivered to the liver was eliminated over this two-week period.
ALC-0315 has no known biology. In the absence of this ‘biological relevance’ the applicant used an estimation of >95% elimination of ALC-0315 to represent the essential elimination from the body. The elimination half-life of ALC-0315 in the liver following IV administration in the rat is approximately 6-8 days. These data indicate that 95% elimination of ALC-0315 will occur approx. 30-40 days following final administration in the rat.
Based on the understanding of the process involved in the terminal half-life, redistribution from tissues into which the lipid nanoparticle is delivered, a similar half-life and time to 95% elimination in human is expected (Mahmood et al, 2010). Examination of the scaling of the comparable lipids (PEG2000-C-DMG, DLin-MC3-DMA) in patisiran indicates that the half-life of these lipids appears to scale with a value approaching the typically used exponent for half-life (0.25). If this is the case for ALC-0315 we may expect a half-life approximating 20-30 days in human for ALC-0315 and 4-5 months for 95% elimination of the lipid (Mahmood et al, 2010).
Note that I cannot find the correct paper (Mahmood et al, 2010), because the EMA’s document is so shoddy that it doesn’t list the references. I looked around a bit, but I’m a bit wary now that ‘even’ I, with my academic background and bespoke ‘literature research experience’, cannot easily find this paper.
Be that as it may, note that these numbers are all derivative. Neither BioNTech nor Pfizer studied anything for more than two weeks, and the EMA correspondingly ‘expects’ that ALC-0315 is almost eliminated after 4-5 months. For a substance whose toxicity hasn’t been studied, this isn’t even close to ‘good enough’, I’d argue.
Where does this stuff go in a human body?
Biodistribution: Several literature reports indicate that LNP-formulated RNAs can distribute rather non-specifically to several organs such as spleen, heart, kidney, lung and brain.
In line with this, results from the newly transmitted study 185350, indicate a broader biodistribution pattern with low and measurable radioactivity in the ovaries and testes. Given the current absence of toxicity in the DART data, the absence of toxicological findings in gonads in the repeat-dose studies and that the radioactivity in the gonads were low (below 0,1% of total dose), the current data does not indicate it to be a safety concern.
So, this stuff ‘distributes rather non-specifically to several organs’, which ‘indicate[s] a broader biodistribution pattern’, and there’s a ‘current absence of toxicity in the DART data’.
Aren’t you rather reassured that this is ‘safe’ for human use?
On Toxicology, there is this:
Although no extensive pharmacological assessment has been conducted in rat (only in mouse and non-human primate), the rat was used as a toxicological animal model in the repeat-dose toxicity studies. The positive neutralization assay results in the repeat-dose toxicity studies demonstrate that V8 and V9 generate an immune response in this species (i.e., SARS-CoV-2 antibodies), partially supporting the use of the rat as an animal model. Other SARS-CoV-2 immune responses in rat remain unclear. The immune responses, especially at the injection sites (e.g., oedema, erythema), seem to increase with each injection in the studies (n=3). There was a marked increase in acute phase proteins, fibrinogen and reduced albumin-globulin ratio (but no increase in cytokines with V8, unclear for V9). There was also a general
increase in immune cells (LUC, neutrophils, eosinophils, basophils) and a decrease in red blood cell parameters (reticulocytes, RGB, HGB, HCT). The spleen was enlarged at both 30ug V9 and 100ug V9 and the draining and inguinal lymph nodes were enlarged mostly at 100ug (V8) but also in a few animals at 30ug (V9)
Thus we depart the realm of science, and entered the realm of ‘The Science’.
Rats are used despite the absence of an ‘extensive pharmacological assessment’. Still, ‘immune responses remain unclear’, and while these ‘seem to increase with each injection’, this document is still (!) cited by Commissioner Kyriakides in February 2022. We’ve since learned about the problems in the lymph nodes an of strange patterns observed with respect to red blood cells, which are, you know, kinda important for humans.
Systemic complement activation (which sometimes may be induced by liposomal drugs and biologicals and potentially result in hypersensitivity reactions) was not investigated as no signs indicative of such clinical manifestations were detected [please, dear semantic scholars, can you interpret this nonsense?]. An absence of dose-response designs in the studies increases the difficulty to interpret the effects. Overall, the V8 and V9 test substances invoked a strong but mostly reversible immune-linked response in rats after 17d exposure. Increases in neutrophils, monocytes, eosinophils and basophils were observed in study 20GR142. For the Applicant, increases in neutrophils, monocytes, eosinophils and basophils observed in the Study 20GR142 were related to the inflammatory/immune response to BNT162b2 administration. Similar findings were also identified in Study 38166 in animals administered 100 μg BNT162b2. The applicant stated that the increases in eosinophils and basophils are a minor component of the inflammatory leukogram, which is dominated by increases in neutrophils. The Applicant also informed that characterisation of large unstained cells was not conducted since the identification of these cells would not provide additional information. The
CHMP agreed with this position.
This paragraph is so full of non-sequiturs and highly questionable statements, I’d say, that it serves merely as illustration of the decay of academic medicine, the EMA, and the private companies that applied for the EUA.
Key take-aways from this section (p. 55):
With regards to the vaccine components, only the whole formulation (modified RNA in LNPs) were used, so there is no toxicological data on the LNP alone or its specific novel excipients. The novel LNP components, these are not considered primarily as adjuvant substances.
No genotoxicity nor carcinogenicity studies have been provided. The components of the vaccine formulation are lipids and RNA that are not expected to have genotoxic potential.
This section is followed by the following paragraph:
The novel excipient ALC-0159 contains a potential acetamide moiety. Risk assessment performed by the Applicant indicates that the risk of genotoxicity relating to this excipient is very low based on literature data where acetamide genotoxicity is associated with high doses and chronic administration (≥1000 mg/kg/day). Since the amount of ALC-0159 excipient in the finished product is low (50 μg/dose), its clearance is high and only two administrations of the product are recommended for humans, the genotoxicity risk is expected to be very low.
I have so many more questions now, as opposed to before my reading of these documents.
Thus, the EMA’s ‘Experts’ Conclude (pp. 55-56)
Some rats intramuscularly administered Comirnaty (receiving 3 full human doses once weekly, generating relatively higher exposure in rats due to body weight differences) developed some injection site oedema and erythema and increases in white blood cells (including basophils and eosinophils) which is consistent with an inflammatory response as well as vacuolation of portal hepatocytes without evidence of liver injury. All effects were reversible. These findings are described in SmPC section 5.3.
As per guidance, no genotoxicity nor carcinogenicity studies were performed. The components of the vaccine (lipids and mRNA) are not expected to have genotoxic potential. This is acceptable to the CHMP.
Finally, the combined fertility and developmental toxicity study showed that SARS-CoV-2 neutralising antibody responses were present in maternal animals from prior to mating to the end of the study on postnatal day 21 as well as in foetuses and offspring. There were no vaccine-related effects on female fertility, gestation, or embryo-foetal or offspring development up to weaning. The CHMP noted that no data are available on vaccine placental transfer or excretion in milk.
Now I’m really curious: who issued the ‘no guidance’ order? The manufacturer’s ‘expectations’ are going to ‘acceptable’? (For a thought experiment, try replacing ‘manufacturer’ with ‘tax office’…)
As regards fertility implications, read that last paragraph again: it has been shown ‘that SARS-CoV-2 neutralising antibody responses were present in maternal animals from prior to mating to the end of the study on postnatal day 21 as well as in foetuses and offspring’. THIS CRAP KNOWINGLY MOVES FROM MOTHER TO CHILD—AND IT IS KNOWINGLY ADMINISTERED TO WOMEN OF CHILD-BEARING AGE.
Having no data and asking for (conditional) marketing authorisation is apparently enough to be ‘noted’. There are no consequences, apparently, to such actions.
The ‘Attached’ Documentation includes another set of insanities that are mind-boggling. Highlights incl.:
Based on the review of clinical data and the above-mentioned reports, CHMP did not identify the need for a GCP inspection of the clinical trials included in this dossier. (p. 57, my emphasis)
There were two then-ongoing immunogenicity studies (BNT162b1 and BNT162b2), which looked at this—some would say crucial—aspect. Turns out that the number of study participants a whooping total of 144 ‘healthy adults aged 18 to 55yrs’ plus another 72 ‘healthy adults aged 56-85 yrs’ (p. 59). The EMA deemed two studies of a total of 216 individuals apparently good enough; in reality, there were even less:
Phase 1 comprised 15 participants (randomization ratio of 4:1 so that 12 received active vaccine and 3 received placebo) per group; 13 vaccine groups were studied, corresponding to a total of 195 participants (the 100 μg dose was only used in the younger adult cohort). (ibid.)
Beginnings and endpoints extend from 21 days before Dose 1 to ‘Day 29 (7 days) after the second vaccine dose’, while ‘functional antibody response’ was only deemed ‘secondary’ (but studied until day 50, all via pp. pp. 59-61).
The worst reading really came on p. 68, entitled ‘Exclusion Criteria’ (my emphases):
Other medical or psychiatric condition including recent or active suicidal ideation/behaviour or laboratory abnormality that increased the risk of study participation or, in the investigator’s judgment, made the participant inappropriate for the study.
History of severe adverse reaction associated with a vaccine and/or severe allergic reaction to any component of the study intervention.
Receipt of medications intended to prevent COVID-19.
Previous clinical or microbiological diagnosis of COVID-19.
Immunocompromised individuals with known or suspected immunodeficiency, as determined by history and/or laboratory/physical examination.
Bleeding diathesis or condition associated with prolonged bleeding that would, in the opinion of the investigator, contraindicate intramuscular injection.
Women who are pregnant or breastfeeding.
Previous vaccination with any coronavirus vaccine.
Individuals who received treatment with immunosuppressive therapy, including cytotoxic agents or systemic corticosteroids, e.g., for cancer or an autoimmune disease, or planned receipt throughout the study. If systemic corticosteroids were administered short term (<14 days) for treatment of an acute illness, participants should not have been enrolled into the study until corticosteroid therapy had been discontinued for at least 28 days before study intervention administration. Inhaled/nebulized, intra-articular, intrabursal, or topical (skin or eyes) corticosteroids were permitted.
Receipt of blood/plasma products or immunoglobulin, from 60 days before study intervention administration or planned receipt throughout the study.
Participation in other studies involving study intervention within 28 days prior to study entry and/or during study participation
Previous participation in other studies involving study intervention containing lipid nanoparticles
In other words: literally anyone who wasn’t fit and healthy to begin with. And to think we’re injecting these into the most vulnerable and high-risk groups first really boggles the mind.
Here’s the endpoints that were studied:

The incidence per 1,000 person-years infected. 7-14 days after Dose 2.
Yep, you read that correctly: 7-14 days.
Why on earth are we even contemplating Covid Passports?
In a sane world, that ‘idea’ would have never arisen.
Hence, it you’ve made it through the previous and this posting, you’re either clearly insane—or ‘they’ are.
Lest you think about questioning your sanity:
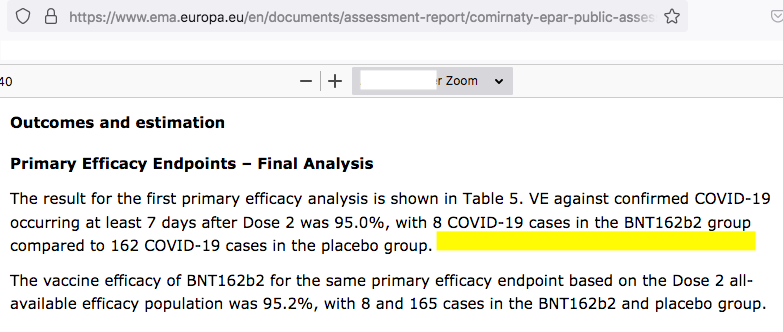
8 vs. 165 cases = 95% vaccine efficacy. Against the wild type. We’re rapidly movig beyond Omicron.
Pull these products.
Ms. Kyriakides, shall we indict your for incompetence or malfeasance?
I’d opt for both.
J’accuse.
"...and only two administrations of the product are recommended for humans." So good to know then that people are lining up where I live for a fifth dose even though it has not yet been approved.
Not insane, criminal. Now that I know that they knew thanks to your investigations, its all the more reason to prepare for a worse case scenario as the fascist global elite will risk the entire planetary human social structure to hide their planetary-scaled crimes.