


Enter the 'Internet of Medical Things (IoMT)'
We all knew this was going to happen, so, perhaps hooking up to the web is the the next stage of development of Transhumanism™

Soon after the Covid poison juice was rolled out, first ‘fringe’ researchers began mentioning strange nano structures, bluetooth signals from humans, and seemingly otherworldly things, such as magnetism on the injection site. What has not been scrubbed from Youtube or Twitter may still be available on Rumble or Odysee.
While I at first dismissed these as crackpot stuff, I soon began to wonder: what if ‘it’ (whatever ‘it’ means) is at least partially true? I mean, at this point in time, we may rather safely declare that many of the most beloved so-called ‘conspiracy theories’ are a bit closer to reality than we might wish that to be the case. I’m not going to point to specifics here (because I don’t want this piece to go there today), hence I merely point out that the ‘intelligence community’ has done so many godawful things since 1945 that it boggles the mind to consider them ‘beyond reproach’.
Rather, today’s piece is connected (pun intended) to a recent paper by IT researchers Shashanu Razdan (School of Computing, National College of Ireland) and Sachin Sharma (School of Electrical and Electronic Engineering, Technological University Dublin), which bears the telling title ‘Internet of Medical Things (IoMT): Overview, Emerging Technologies, and Case Studies’ and appeared in IETE Technical Review vol. 39, no. 4 (2022).
I’ve removed the references (for readability) and added my own emphases [and, occasionally, snarky commentary]. Down this particular rabbit hole we go, shall we?!
Abstract
In the Internet of Medical Things (IoMT), the Internet of Things (IoT) is integrated with medical devices, enabling improved patient comfort, cost-effective medical solutions, quick hospital treatments, and even more personalized healthcare. The paper first provides the introduction of IoMTs and then introduces an architecture of IoMTs. Later, it provides the current operations of the healthcare system and discusses the mapping of these operations into the architectural diagram. Further, several emerging technologies such as Physically Unclonable Functions (PUF), Blockchain, Artificial Intelligence (AI), and Software-Defined Networking (SDN) are envisioned as important technologies to overcome several challenges in e-healthcare such as security, privacy, accuracy, and performance. Finally, we provide three case studies for IoMT based on – (1) PUF-based Authentication, (2) AI-enabled SDN Assisted e-healthcare, and (3) Blockchain Assisted Patient Centric System. The solutions presented in this paper may have a huge impact on the speed at which IoMT infrastructure can efficiently evolve with market evolution.
Are you intrigued yet?
What, then, is the ‘Internet of Medical Things (IoMT)’?
The Internet of Medical Things (IoMT) is the blend of medical devices with the Internet of Things (IoT). IoMTs are the future of current healthcare systems where every medical device will [I take it this means no opt-out] be connected and monitored over the Internet via healthcare professionals. This offers a faster and lower cost of health care as it evolves. Figure 1 shows an example of IoMTs where patient vitals are collected via sensor devices and sent to the IoMT applications through the Internet. The information then flows to the healthcare expert and medical staff and then a response is sent back to the neededpatients [sic].
Here is Figure 1:
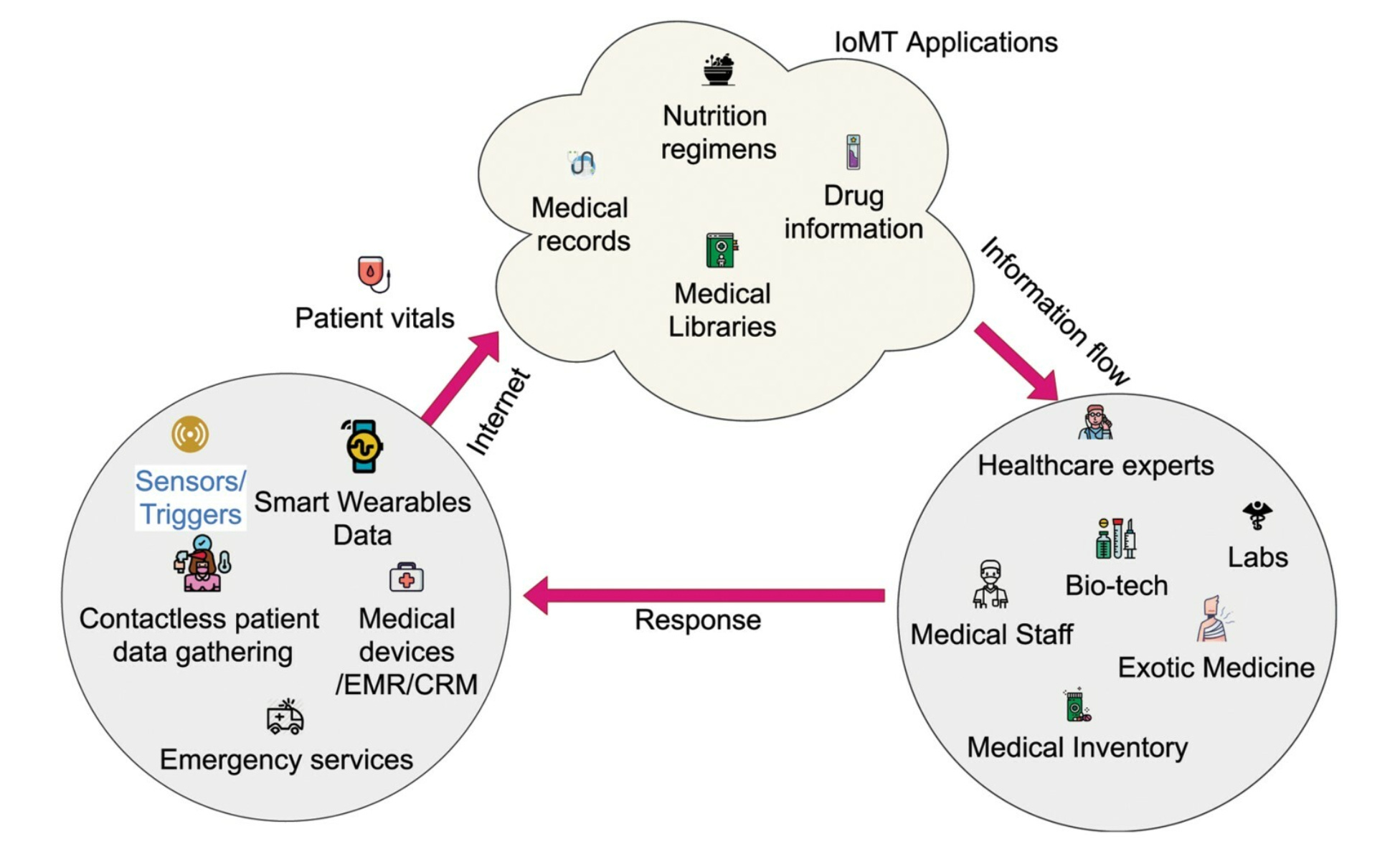
Note in particular the ‘sensors/triggers’ and the ‘contactless patient data gathering’, with the latter quite likely not referring to thermometers taking body temperature. Let’s not forget about the ‘medical devices’, such as, I presume, implants that will also be connected to the internet.
And the next section is where we’ll more clearly get told what to expect in the near-future:
During COVID-19 pandemic, there is currently a rise in telehealth practices due to physical distance guidelines which are compelling healthcare professionals to operate patients remotely through IoMT devices [as if this ‘rise’ fell out of a blue sky one Monday morning]. Further, Sustainable Development Goals (SDG) by 2030 was approved by the United Nations (UN) in 2015 [oh, look, another of these crazy conspiracy theories to muse about]. Good health and well-being is an important goal in SDG [this prose is about as complex as George W. Bush ‘splainin’ whatever]. Currently, IoMT has the ability to fulfil the goal of good health and well-being [which is why we’ll be forced to implement it]. This paper is about providing an overview of IoMT, listing and presenting important emerging technologies such as Physically Unclonable Functions (PUF), blockchain, Artificial Intelligence (AI) and Software-Defined Networking (SDN) in IoMT, and providing case studies of IoMTs. The contributions of this paper are as follows:
Introducing a Cloud-Fog architecture to IoMT.
Presenting review work on PUF, blockchain, AI, and SDN for e-healthcare.
Proposing PUF, blockchain, AI, and SDN-based mapping for e-healthcare.
Providing an experimental study to the case studies considering the above mapping in IoMT.
And this brings us to Section 2.1, which is entitled ‘IoMT and Enabling Wireless Technology’. It reads as follows:
IoT systems consist of sensors and devices connected via a network of cloud ecosystems over high-speed connectivity between each module. The raw data collected at these devices/sensors is sent directly to the vast storage offered by cloud services. This data is further cleaned and then analysed to gain further insights into it. This requires additional software, tools, and applications which will further assist in visualization, analysis, processing, and management of the data.
Figure 2 shows several wireless technologies such as RFID (Radio Frequency Identification), NFC (Near Field Communications), Bluetooth, LTE (Long Term Evolution) and 5G/6G (and beyond) inter-linked with several devices such as smartphones, monitoring devices, sensors, smart wearable, and other medical devices. Currently, the use of 5G/6G or beyond is prevalent in IoMT [huhum, 5G isn’t fully rolled out, and they are talking about 6G? It doesn’t (yet?) exist: would that be another ‘conspiracy theory’?] due to their high bandwidth and ultra-low latency benefits.
Here’s a 2021 paper on 6G technology if you care that much about it. It’s not operational, and research and testing, while ongoing since around 2005, isn’t prevalent (yet). 6G is supposedly to be rolled out by 2030.
Here’s Figure 2:

Basically, the IoMT is an unholy union of wirelessly inter-connected monitors and God knows how many people, certainly AI ‘services’, and whatever else is deemed ‘advantageous’.
Moreover, these wirelessly inter-connected monitors etc. will be paired with ‘Smart Hospitals’:
Smart hospitals are the hospitals that are built on intelligent automated and optimized modules (maybe based on AI/ML) on the ICT infrastructure to improve patient care procedures and to add new capabilities. There are several applications of smart hospitals such as telemedicine, telehealth, remote robot surgery. Telemedicine is to provide clinical care at a distant location, while telehealth is to provide non-clinical care at a distance. In remote robot surgery, medical robots perform surgery through instruction from the doctor sitting far away…
Inbound data from various sources is first collected (e.g. through remote gathering or physical gathering) and sent to EHR (Electronic Health records systems). Data could be classified as unstructured if it is collected offline on paper as medical notes by the personnel. If the data is collected in a structured form from the devices and sensors by using predefined data fields for users to enter, then it becomes easy to process in further systems such as CRM (Customer Relational Management) System [yee-haw, New Public Management will do all of this]. The CRM brings to use the tools for analysing data and then assigning it to its predefined target in the ecosystem. The essential data and information from EHR systems is sent to the CRM system and it processes this patient data. This processed data generates further triggers to patients and medical personnel in the ecosystem [this looks like Skynet for the healthcare sector; remember, there’s likely no opt-out other than a loaded shotgun getting rid of the drone ‘reminding’ you of your umpteenth modRNA posion juice ‘update’]. The patients receive outbound communication from hospitals and health experts in the form of personalised health regimens [ah, it will look individual but in reality it’ll be all centralising bureaucracy; reeks of collectivism]. The doctors and other medical staff get notified about the reminders and other alerts from the same CRM software in the ecosystem [and, as Leonard Cohen sang, ‘everybody knows’ about your health status].
There but one question: what can go wrong?
The Architecture of the IoMT
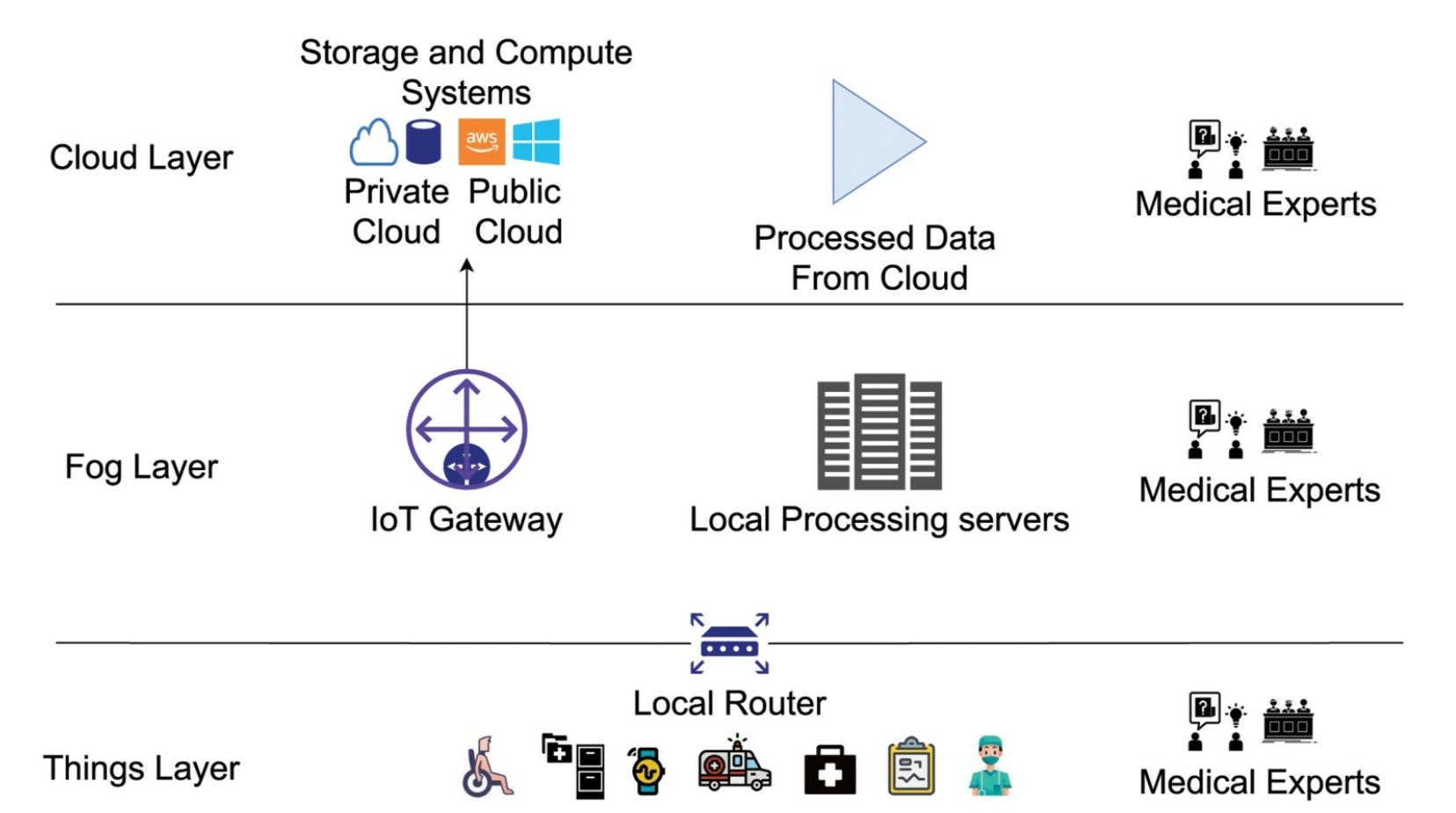
The architecture for IoMTs consists of three layers (Figure 4). There are three layers: (1) things layer, (2) fog layer, and (3) cloud layer…healthcare experts can also communicate directly through the router between the Thing layer and Fog layer and through the local processing servers at the fog layer [no need for patient rights, of his concern, with data protection, which is a term that’s notably absent here]…
The things layer consists of patient monitoring devices, sensors, actuators, medical records, pharmacy controls, nutrition regimen generator, etc [i.e., everything plus the kitchen sink]. This layer is directly in contact with the users of the ecosystem. The data from elements such as wearables, patient-monitoring data, remote care data is collected at this layer…data is further processed at the fog and at the cloud layer to generate meaningful information. Further, in order to reduce the delay, the healthcare experts can get the patient data…
The fog layer operates between the cloud and the things layer. This layer consists of local servers and gateway devices for a sparsely distributed fog networking framework. The local processing power is harnessed by the lower layer devices for real-time response to their users…to reduce the delay, the healthcare experts can get the patient data through this router.
The cloud layer consists of data storage and computation resources for the data to be analysed and derive decision-making systems based on it [112% this will be ‘assisted’ by ‘AI’; imagine, for once, the situation where you find yourself sitting in a GP’s office and the physician tells you that you’re overweight or consume too much alcohol—based on such ‘fog and cloud computing’—, thereby your copays are higher]. The cloud also offers a vast reach to incorporate huge medical and healthcare systems to handle their day-to-day operations with ease [it’s a grift, plain and simple]. This layer consists of cloud resources where the data generated from the medical infrastructure will be stored and analytical work could be performed as deemed necessary in the future [so what the authors want is a blank cheque to monkey with user/patient data ‘as deemed’—by whom? for whose profit?—‘necessary’].
Here’s Fig. 4, entitled ‘operations within layers in IoMT’:
What About Future Prospects?
There are several options mentioned, incl. ‘blockchain, PUF, AI, and SDN’. I’ll delimit myself to a few choice quotes:
Blockchain offers a solution to many issues arising in the security of participating entities in the healthcare system built around it.
If you think that any blockchain-dependent entity offers no options of monkeying with data and/or backdoors, think again. About Bitcoin and CBDCs, for instance.
Physically Unclonable Function (PUF) devices generate a unique fingerprint for the vulnerable elements in the IoMT ecosystem…after the fog layer, security is ensured by more specialized enterprise security solutions offered by service providers in the architecture
I read this as permitting identification of individuals, all ‘safeguarded’ by IT security firms, perhaps as ‘good’ ones as, say, CloudStrike.
Applications of AI, including Machine Learning (ML) and Natural Language Processing (NLP) in e-healthcare. Precision medicine requires advanced diagnostics and tailored regimens with quick delivery time. AI makes a compelling case for this by offering real-time solutions in determining new pathways for treating certain conditions based on historic and real-time data.
This is actually the only aspect where ‘AI’ looks ‘better’ at making correct diagnoses relative to humans (‘problem’ is, though, that biology and biological markers, such as sex, are identifiable, e.g., see Rachel Gordon’s ‘Artificial intelligence predicts patients’ race from their medical images’ via MIT News from 2022, which the politically correct morons call ‘bias’.)
The network part in IoMTs can be divided into two parts: (1) data plane and (2) control plane. The data plane forwards traffic towards its destination, while the control plane performs the necessary tasks that allow the data plane to make forwarding decisions. Software-Defined Networking (SDN) provides a standard way to communicate between the data plane and control plane…This interface is important for the collection of data from the control plane and the insertion of commands from the AI application to the IoMT device. The proposed architecture is a modified version of the architecture proposed for the Internet of Vehicles enabled with SDN.
The remainder of the paper consists of descriptions of various ‘case studies’ that show how far these various features are already implemented, albeit in a non-networked way.
Bottom Lines
Remember the dystopian movies of yesteryear, from ‘The Matrix’ to ‘The Network’ to ‘Terminator’. This is soon coming to your GP’s premises.
If these trends continue—which seems likely—we’ll get the worst of all possible worlds, with ‘biases’, such as biology and the like, removed because those who pay for these ‘services’ are easily offended by ‘AI’ determining, e.g., racial features.
Once implemented in a ‘trial run’, politicos and business people will point to the excess costs of going back to any kind of ‘previous’ systems. ‘Journos™’ will happily offer their (prostituting) services to politicos and big business.
Of course, this won’t end well, most likely in a way as shown in ‘Elysium’ feat. Matt Damon, which incl. this infamous scene of the latter’s character ‘talking’ with a ‘healthcare robot’ interface.
We’ll look at these things in more detail next week.
In the meantime: beware the ‘good intentions’ of electronic patient records.
This has been discussed on the principle-level since the 1960s, I have to point out.
Always with a rephrased eugenicist agenda.
Tracking chips to find lost people and fugitives. Enhancers and monitors of different kinds, f.e. for diabetics and epileptics. Thought-controlled machinery (already semi-possible).
And ne'er a thought from the modernist-futurist technophiliacs about the sad Iron Law of technology:
Any and all technology will always be pushed to its technical limitations, before human limitations are applied to it.
As I've used an example when in class: first, the car came. Then modern roads. Then traffic wardens/lights and crossings. Then rules for cars and driving. The licenses. And so on. Young people are often stunned to learn that it is within living memory that drunk driving was up to the intercepting officer to decide, and that a set limit in parts per thousand is in many nations a 1980s invention, or even later than that.
Now then, a species who takes a century to come around to realising that driving a 60-ton logging truck while inebriated is a Bad Thing(tm), is such a species to be trusted with hooking their brains up to machinery?
"Remember the dystopian movies of yesteryear, from ‘The Matrix’ to ‘The Network’ to ‘Terminator’. "
Let's also not forget 'Idiocracy'.