


Covid in Norway: 'all-cause jabbed' are leading hospitalisations, ICU admissions, deaths, esp. pronounced among 'boosted' individuals
Still, domestic and EU policies on Covid Passports will all but ensure Norwegians will continue to line up to get a third injection, all evidence to te contrary by damned

In yesterday’s post, we discussed the Institute of Public Health’s (IPH) risk assessment, which showed a number of oddities as well as continuities. Here are the main take-aways:
(mass) testing will end soon, having outlived its usefulness.
Mandates don’t work, hence it’s time to end them.
Most pressure will fall on the first providers, even though the IPH expects 3-4m infections.
Despite all this, still (!) no mention of early treatment.
So, in all a mixed bag of goods, and yesterday we discussed the data in the main part, some of it is worth repeating to prepare the ground:
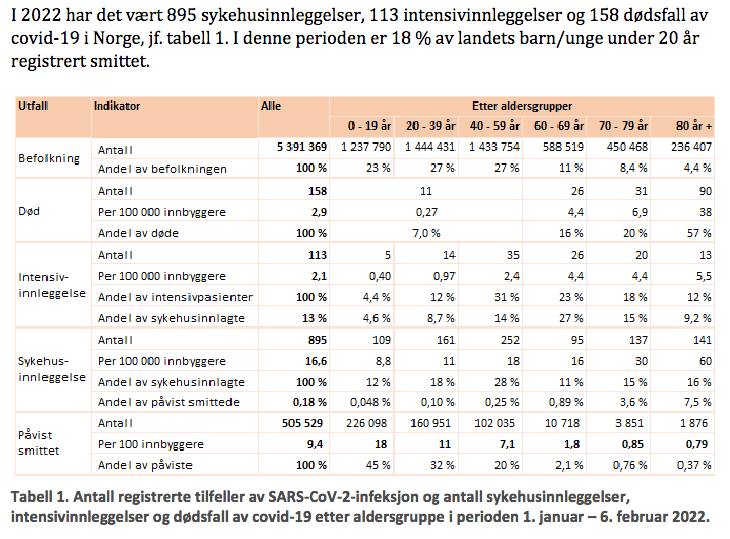
Covid is a bad thing, if you’re 60+ years, who constitute 23.8% of Norway’s population.
93% of all Covid-associated deaths, 53% of all such ICU admissions, and 42% of all hospitalisations occurred among this particular demographic.
Yes, these can be broken down further, as shown by Table 1 (p. 9), reproduced below: the older you are, the more likely you are to be in harm’s way (doh).
Given the less-than-severe demonisations of all ‘unvaccinated’ in Norway relative to other places (here’s looking at you, Covidistan), it does make one wonder why the legacy media and some other less-reputable individuals (such as the women I encountered last week) engages in such disgusting amounts of fear porn agit-prop (e.g., here), instead of looking at these numbers and call for the elderly to be put into special housing units, keep under lock-down for years on end, and blame them for getting sick (/sarcasm).
I mean—just look at the numbers (based on Table 1 above, computed via a presumed case fatality rate, or CFR, as follows: no. of deaths X 2 / no. of ‘cases’)
60-69: CFR = 0.0048
70-79: CFR = 0.016
80+: CFR = 0.0959
In all, really small numbers, but they are much, much, much larger than, say, for everyone below age 60 (CFR = 0.00004498), but guess what: 158 deaths of Covid-19 in these past five weeks are almost negligible, esp. if related to other human activities that can be considered ‘regular’ activities, such as driving a car.
Also, if you’re among the weak-hearted (no pun intended, my dear jabbed’n’boosted neighbours), the following is a good old-fashioned ‘let’s compare apples and oranges’ kind of argument, which does have merit, I’d argue:
How do these rates compare? Well, according to the Norwegian State Statistics Bureau (SSB), the five-year average number of people killed on Norway’s roads in 2021 was 110, the number of injured (presumably requiring hospitalisation) was 623, which is the number for the entire year, i.e., it’s a bad comparison. As an aside, guess what: these numbers also skew considerably by age (older people are a bit more at-risk of dying than younger people) and gender (many more men died compared to women).
Sidenote: I did some more digging on the SSB’s website and found some more data points that allow for a somewhat better comparison. According to data point 12043 (Persons killed or seriously injured, 2015-2019, i.e., all pre-Covid), these yearly numbers of roadkill (harr) stood between 106 (2017) and 135 (2016), so for a broad average, divide by 12 and compare to the 158 Covid-associated deaths in early 2022 so far.
If you’re even more into this, you’ll like the following, too. I also checked the monthly figures for Jan. 2015-2019 (see here), and guess what: there’s like only zeroes in the database. This allows us to conclude, yes, Covid-19 is much, much more dangerous than driving a car in Norway, and it skews precipitously towards the elderly. You know, like driving, but even more so.
With this settled, let’s take one more look at that above table before we move on: check out the bottom three lines (‘påvist smittet’, or ‘confirmed cases’): 45% of all registered ‘cases’ occurred among 0-19yo, 32% among the 20-39yo, and 20% among the 40-59yo. In sum, 97%, but consider the fact that 93% of all fatal outcomes accrue in ‘the other 3%’ of the population.
Let that sink in: as I’ve said earlier, Norway’s done an admirable job of ‘protecting the elderly’, which, if these data are kinda correct, are at really high risk from Covid-19, hence the recommendation to abrogate all mandates—for everyone else—in the face of Omicron.
One last aspect to note: I’d still like to learn all the details possible about the co-morbidities of those hospitalised for Covid-19, which is the one data point that’s consistently missing (but, perhaps, we’ll get that piece of information in, say, 2045).
Updates for Weeks 4 and 5
The below sources can be found here (week 4) and here (week 5). Apologies for the ‘missing’ update from last week: too little time, too much going on over in Covidistan, and offline life (work) deadlines intersected.
Over the past couple of weeks, hospitalisations have increased and appear to be on a plateau right now, as shown in Fig. 3 (p. 10, week 5), and they did so at about the same level of 2021 (and slightly lower than before Christmas last year), albeit the large increase you can see about a year ago occurred slightly later.

Sidenote: you know, I can’t help, but these data appear a bit odd in terms of Covid’s presumed seasonality, which suggested that these ‘waves’ (bølge) should be occurring during ± the same period each year, right? Instead, the first wave of hospitalisations crested in mid-April 2021 (that yellow arrow on the left), and the other wave crested in the week after Christmas 2021 (the yellow arrow on the right), which is odd as they are apparently out of sync with every other indicator, incl. mortality, which of course also relates to seasonal occurrence of Covid-19.
So, I ventured further down the rabbit hole and checked OWID if there’s something else to consider. Behold, according to OWID, first-dose uptake exploded right around the same time in mid-April 2021, so that above first wave conicided with the explosion of injection uptake, incl. the crucial two-week post-injection window, which means that ± all adverse effects would be counted among ‘the unvaccinated’.

No such patterns after the second dose, though, with perhaps the 70-79yo age cohort as a partial driver of the above-mentioned wave.

But look at the booster (third dose) uptake, which—much like the first dose—accelerated at about the same time these hospitalisations peaked.

Now, I don’t mean to suggest causation here, but these data points appear quite closely correlated in time and space, in particular once we factor in the 14-day post-injection obfuscation that considers whatever follows these injections happens to ‘unvaccinated’ (post dose 1) or ‘not-yet fully vaccinated’ (after dose 2).
In a sane world, I’d expect, say, the government, public health authorities, and, yes, legacy media to enquire about this. But they don’t, hence me sitting here and typing this, and you, my dear reader, looking at my musings.
This is a long post, again, already, so I’ll skip over many interesting details and present you with the main trend I terms of hospitalisation for Covid-19 (fig. 7, p. 14, week 5), which sums up the state-of-play quite nicely:

As you can see, the trend line for the ‘unvaccinated’ has been steadily declining since—week 51, i.e., the moment boosters were made available for everyone in the age brackets 45-64. What a coincidence, isn’t it?
At the same time, the trend line for ‘jabbed’n’boosted’ (recipients of 3 doses) continues to seemingly inexorably rise. Last week, ‘fully vaccinated’ (2 doses) constituted the single-largest group among those hospitalised for Covid-19, by week 5, ‘jabbed’n’boosted’ is firmly in the lead. Here are the numbers:
Week 4, pp. 11-12: of 200 new admissions, vaccination status was known in 181 cases: 56 (31%) were ‘unvaccinated’, 61 (34%) were ‘fully vaccinated’ (grunnvaksinert), and 58 (32%) had received three doses; there were also 3 ‘partially vaccinated’ (i.e., 1 dose, but after 21 days) and 3 more ‘partially vaccinated’ but within that 21-day window.
Week 5, pp. 12-14: of 215 new admissions, vaccination status was known in 194 cases: 59 (30%) were ‘unvaccinated’, 43 (22%) were ‘fully vaccinated’ (grunnvaksinert), and 76 (39%) had received three doses; there were also 14 ‘partially vaccinated’ (i.e., 1 dose, but after 21 days) and 2 more ‘partially vaccinated’ but within that 21-day window.
So, in other words: four out of ten admissions are those who received three doses, which, as discussed above, are primarily among the middle-aged to elderly (45+); another two out of ten admissions were double-jabbed patients. By contrast, only three out of ten were among the unvaccinated, whose age ranges are lower. The remaining one out ten admissions is among the ‘partially vaccinated’, i.e., from those cohorts who received one dose ‘only’.
This is summarised in Fig. 6 (p. 13) below:

As my highlights show, do pay good attention to the past four weeks data (siste 4 uker, highlighted in yellow), for the numbers are quite striking:
Hospitalisations (Sykehusinnleggelser): 220 ‘unvaccinated’ vs. 173 ‘fully vaccinated’ (grunvaksinert) vs. 224 ‘fully vaccinated and boosted’ = 64% of all hospitalisations affected ‘all-cause vaccinated’ individuals.
ICU admissions: 20 ‘unvaccinated’ vs. 15 ‘fully vaccinated’ vs. 9 ‘fully vaccinated and boosted’ = 55% of all ICU admissions affected ‘all-cause vaccinated’ individuals.
ICU admission plus ventilator: 17 ‘unvaccinated’ vs. 15 ‘fully vaccinated’ vs. 6 ‘fully vaccinated and boosted’ = 55% of all ICU admissions plus ventilator affected affected ‘all-cause vaccinated’ individuals.
Now, please look at the moderate-to-high risk group categorisation (the last column on the right), and let’s check out these numbers, too:
Hospitalisations: 56 (17.5%) ‘unvaccinated’ vs. 82 (26%) ‘fully vaccinated’ (grunvaksinert) vs. 182 (57.5%) ‘fully vaccinated and boosted’ = 64% of all hospitalisations affected ‘all-cause vaccinated’ individuals.
ICU admissions: 7 (32%) ‘unvaccinated’ vs. 8 (36%) ‘fully vaccinated’ (grunvaksinert) vs. 7 (32%) ‘fully vaccinated and boosted’ = 68% of all hospitalisations affected affected ‘all-cause vaccinated’ individuals.
ICU admission plus ventilator: 6 ‘unvaccinated’ vs. 8 ‘fully vaccinated’ (grunnvaksinert) vs.—n/a ‘fully vaccinated and boosted’, which aren’t specified here ‘due to data privacy concerns’ (this is the ** note, but given the awful numbers discussed above, I don’t know if I’d like to know that one).
One (appropriately the) last word from this weekly update concerns—deaths (pp. 19-20, week 5), from which the below Fig. 9 is taken:

While the past four weeks there’s information on 113 Covid-associated deaths, only a mere 31 (27.4%) of these occurred among ‘the unvaccinated’, with the overwhelming majority of them—78 (69%) among ‘all-cause vaccinated’; to this number, add another 3.5% who were ‘partially vaccinated’. In other words: the share of Covid-associated deaths—as is the case with hospitalisations—is roughly in line with Covid injection uptake (c. 72% with two or three jabs, plus almost 6% with ‘at least on dose’, according to OWID).
Also note that there were 49 Covid-associated deaths who received a ‘booster injection’. 49 of these 113 deaths are…43% of all Covid-associated deaths in the past four weeks are also roughly in line with the share of the Norwegian population who received a booster injection.
Note further that these 49 Covid-associated deaths are 63% of all ‘fully vaccinated and/or boosted’, which is a share that actually exceeds the share of the Norwegian population who received a booster injection.
Finally, note that the total numbers given in Fig. 9 only tell you cumulative deaths since the injections were rolled out on 28 Dec. 2020. As I’ve explained elsewhere in detail, context matters enormously:
From 28 Dec. 2020 to week 39 (2021), there were 61 ‘fully vaccinated’ and 15 ‘partially vaccinated’ Covid-associated deaths for a combined ‘all-cause vaccinated’ total of 76.
This means only one thing: the number of Covid-associated deaths for the ‘all-cause vaccinated’ exploded from late summer onwards:
From week 39 (2021) through week 1 (2022), these numbers rose to 404 ‘fully vaccinated’, 29 ‘partially vaccinated’, and by now also incl. 44 ‘fully vaccinated and boosted’ Covid-19 associated deaths, which provides a combined total of 477.
And to these numbers we may now add the numbers for weeks 2 through 5 (2022): ‘unvaccinated’ deaths rose by 31, as opposed to ‘all-cause vaccinated’ deaths, which rose by 78. In other words: the ‘all-cause vaccinated’ death-rate from Covid is 152% higher than that of the ‘unvaccinated’. (At one later point in time, I’ll put these numbers in a nice-looking gfx, for now please bear with the numbers.)
Conclusions and Outlook
So, where are we?
The government, based on the IPH’s advice that the mandates are harming society more than they are useful, will end most, if not all, (domestic) mandates shortly.
Still, in terms of foreign travel, Norwegians will have to abide by EU rules concerning the Covid Passports and their validity: 180 days for ‘recovered’ (irrespective of injection status), 180 days for ‘fully vaccinated’ (two jabs), and 270 days for those who got a third injection.
Furthermore, local governments all over Norway are mulling plans to end testing (finally), but if a Norwegian resident is planning to travel abroad for leisure, costs (of currently some 250 € per PCR test) will have to borne by the population. (So far, it was taxpayer-financed, i.e., also paid by the residents, but from now it’ll be borne by any individual.)
Consequently, and in all likelihood without taking even the briefest moment to read through the data discussed above, most Norwegians will continue to roll up their sleeves and get a third injection, if only to be able to travel abroad a bit more cheaply.
As a main consequence, I expect the ‘fully vaccinated’ (two doses) group among hospitalisations etc. to plummet further—most will go for the third injection, thus further driving the dynamic, which will inexorably result in much higher rates of hospitalisations, ICU admissions, and death among the ‘fully vaccinated and boosted’ group.
As an aside, since ‘Omicron’ appears very much to be deep in OAS/ADE territory, it’s also quite likely that the share of ‘unvaccinated’ will drop further until it might bottom out at roughly the share of ‘unvaccinated’ among the general population. At that point, the vaccinators will cease talking about injections; if, God forbid, the injected are at even higher risk of (re-) infection relative to the ‘unvaccinated’, then the premium on the latter for working in key positions will become immense.
This will not end well.
My personal take is—dark: only once (quite likely a ‘when’, not an ‘if’) more and more injection-derived consequences in terms of casualties and fatalities will occur, these aspects may change.
You asked about known comorbities. While I can't get you the numbers for Norway, I can check the swedish intesive care registry. However, the text is all in swedish so I'll summarise the most common comorbidites if that's okay?
[https://www.icuregswe.org/data--resultat/covid-19-i-svensk-intensivvard/]
# of ICU patients stands at 8 914 patients from March 2020 to today.
Most common comorbidities (excluding advanced age) are given as:
chronic cardiac/lung disease 29.1%
chronic liver/kidney disease 6.8%
diabetes 25.2%
hypertoni 43.1%
The share of the total number of ICU patients having any comorbidity is stated as 80.6%.
To get more detailed data, one would have to work in health care to have access to more details (and if I had that I would not be allowed to share it publicly anyway due to patient/health care confidentiality) or to be a researcher appointed by legal authority to investigate and again not be allowed to share any data until the report was complete and approved for publication.
As Norway and Sweden are very much alike when it comes the health of the general indigenous population, the proportions in Norway should be similar to those in Sweden.
Thank you for your continuing coverage of the issue. Oh, by the by, some of our regime loyal media has reported that the death toll in Austria is so high that hospitals in Oberösterreich (their spelling) must stack corpses in corridors... Somehow, I find that a little hard to believe, not only because no named austrian source is given, not even the name of a hospital.
And we are realeased. Infected kids can even go to school if fever free, so it is basically saying that we do not care anymore.
It would be hopeful if it was the first time it happens, but they actually did the same last September, and we got three months. I understand perfectly why they decided to close again, and I do not see why the situation is different this time.
Last September they thought that with everyone vaccinated with a "95% or more effective", if people caught it there would be no issues. We all saw that was not the case. Now they are expecting that after a recent omicron infection you have some form of immunity. There are reports already going around that that immunity is not obtained by vaccinated persons. I hope that is not the case in most cases because if not we are in for a big surprise.