
Notes From the Upside Down XVI: a bunch of humanities and social science scholars assessed Sweden's pandemic policies, showing irresponsibility and (likely) criminal intent
Main features incl. 'secrecy, cover-up and manipulation of data…revealed several structural problems in Swedish society' on all levels, incl. the administration of morphine to elderly people

Humanities & Social Sciences Communications, a ‘subsidiary’ of Nature.com, has a new article out. Entitled ‘Evaluation of Science Advice During the Covid-Pandemic in Sweden’, the authors are Nele Brusselaers, David Steadson, Kelly Bjorklund, Sofia Breland, Jens Stilhoff Sörensen, Andrew Ewing, Sigurn Bergmann, and Gunnar Steineck, with the piece appearing in no. 9, art. No. 91 (2022).
From the Abstract
Sweden was well equipped to prevent the pandemic of COVID-19 from becoming serious. Over 280 years of collaboration between political bodies, authorities, and the scientific community had yielded many successes in preventive medicine. Sweden’s population is literate and has a high level of trust in authorities and those in power. During 2020, however, Sweden had ten times higher COVID-19 death rates compared with neighbouring Norway. In this report, we try to understand why, using a narrative approach to evaluate the Swedish COVID-19 policy and the role of scientific evidence and integrity. We argue that that scientific methodology was not followed by the major figures in the acting authorities—or the responsible politicians—with alternative narratives being considered as valid, resulting in arbitrary policy decisions. In 2014, the Public Health Agency merged with the Institute for Infectious Disease Control; the first decision by its new head (Johan Carlson) was to dismiss and move the authority’s six professors to Karolinska Institute. With this setup, the authority lacked expertise and could disregard scientific facts. The Swedish pandemic strategy seemed targeted towards ‘natural’ herd-immunity and avoiding a societal shutdown. The Public Health Agency labelled advice from national scientists and international authorities as extreme positions, resulting in media and political bodies to accept their own policy instead. The Swedish people were kept in ignorance of basic facts such as the airborne SARS-CoV-2 transmission, that asymptomatic individuals can be contagious and that face masks protect both the carrier and others. Mandatory legislation was seldom used; recommendations relying upon personal responsibility and without any sanctions were the norm. Many elderly people were administered morphine instead of oxygen despite available supplies, effectively ending their lives. If Sweden wants to do better in future pandemics, the scientific method must be re-established, not least within the Public Health Agency. It would likely make a large difference if a separate, independent Institute for Infectious Disease Control is recreated. We recommend Sweden begins a self-critical process about its political culture and the lack of accountability of decision-makers to avoid future failures, as occurred with the COVID-19 pandemic.
Lots of interesting stuff in here, dare I say, shall we have a look? And by ‘interesting’ I mean ‘of interest to the state prosecutor’.
Sidenote: textual, or discursive, analysis is very much up my professional alley. As you may recall, I’m a historian working on Europe’s post-medieval past, hence I feel extra qualified to take a look. So, why don’t you come along for the ride as we go through this paper?
Editorial note: I removed most references; if not noted otherwise, all emphases below are mine.
Points of Departure [Introduction]
Let’s read from the paper directly to understand what the authors’ points of departure are:
When the COVID-19 pandemic hit Europe, this sparsely populated Nordic country stood out from the beginning, with an apparent unhurried and less restrictive strategy compared to the rest of the continent. Several sources highlighted ‘Swedish exceptionalism’ as the underlying reason for this diversion, going against international and scientific advice. While other European nations went into strict lockdown mid-March, Sweden banned public gatherings of >500 people, and >50 at the end of March. Officially, the Swedish strategy was centred around individual responsibility, and not overwhelming healthcare systems…The Swedish strategy has been principally based on recommendations and voluntary measures, for example working from home for those who could; yet no legal restrictions (including fines) were enforced during 2020.
So far, this also applies to Norway, by the way. Apart from these issues of ‘like-mindedness’ among Nordic neighbours, the key hypothesis may be summarised as: Sweden acted differently from virtually everyone else, so let’s see why this was done.
In terms of underlying source material, the authors surveyed ‘a large body of internal documents and public statements from various officials during 2020’, albeit only indirectly, citing Lindström, 2021; Nygren and Olofsson, 2021; Orlowski and Goldsmith, 2020; Habib, 2020; Giesecke, 2020; Sörensen, 2020, 2020e; Vogel, 2020; Larsson, 2021.
Furthermore, the source base consists of ‘email conversations and statements from the State Epidemiologist [Anders Tegnell] and others’ that purportedly show ‘that they at least speculated on the use of children to acquire herd-immunity, while at the same time publicly claiming children played a negligible role in transmission and did not become ill’. This is done, again, via indirect citations of Vogel, 2020; Bjorklund and Ewing, 2020; Brusselaers et al., 2020.
Funny enough, the concluding paragraph of the paper’s introduction reads like any undergraduate thesis I’ve surveyed (note that I’m not making fun of hard-working undergraduates, but that my vitriol is rather directed against the supposedly ‘grown-ups’ who make up the authors of that paper):
As a comprehensive evaluation [1] of the COVID-19 policies and implementation in Sweden goes beyond the length and scope of this paper [2], we focus on the role of scientific evidence for the actions using a narrative approach [3]. In this report, we aim to assess [4] the extent to which Sweden had a pandemic strategy before 2020 and how this strategy was based on science [5] and how it has been implemented and adapted into policy making [6] during the pandemic, focusing on the period until December 31, 2020 [7]. We also assess the extent [8] to which scientists, policy makers, and politicians have been involved in the decision-making process. The study is not intended to advance policy or social science theory [9].
Couple of issues:
Why say that before…
Claiming you won’t deliver? This is an illogical (half-) sentence and should have been commented on by the reviewers. The first rule of paper-writing is: be precise about what you’re not doing, and this opening (half-) sentence is misleading.
Hopefully there’s something tangible, or at least helpful in the methods section; I’m a humanities scholar and I don’t know what ‘a narrative approach’ is: are there also ‘alternative’ such approaches? Do we talk discourse analysis (i.e., counting words), semantics, or literary theory? Come on, people, this is ridiculous.
Why a ‘we aim to…’ statement? State your case, as in, e.g., ‘we show’ or the like. This is also paper-writing 101, and, somehow, I get the impression the authors never really thought about, you know, writing.
Next—without a definition of ‘science’, this is equally insulting to my intellect. Do we talk ‘scientific consensus’ (which I find an oxymoron, as science advances by going against the grain) or what else? Throwing around big words and waving hands doesn’t show you’re actually up to the task.
Sure, ‘implementation’ and ‘adaptation’ are quite big buzzwords in the current humanities and social sciences. Typically, it’s just that: reading primary materials from ‘big men’ (and some women) to discern what drove their ‘motivation’ or the like. It’s what History was like from around 1800 to the middle of the 20th century, i.e., a limited number of actors whose writings are usually ‘read against the grain’ and ‘analysed by looking between the lines’. I’ve reviewed countless scholarly volumes for professional journals by now whose author spend 250p. on ‘theory’, add 30p. of ‘analysis’, and come to preposterous conclusions, all without differing significantly from the word-salad espoused above.
At least we get a (presumed starting point in March 2020 and) an end point.
See my comment no. 7 above.
Curiously, no-one asked the authors to do so, but why do they mention this? Here, my personal take may be summarised as follows: someone only mentions such a thing, if that person wants to engage on these terms. Of course, the authors wish to do just that.
Sidenote on no. 9—epimetheus’ first axiom of communication: if someone states that they don’t want to address this or that issue, it is typically the case that this person wishes to do so. E.g., if we meet casually and I ask: ‘how do you do?’, I’m not at-all interested in your answer—I want to be asked how I am faring.
A ‘narrative approach’: Methodology
I kid you not—here’s what the authors write (Italics in the original):
Sweden is a monarchy and the largest country among the Nordic countries, bordering Finland, Norway, and Denmark. The Nordic region is a geographical and cultural region in Northern Europe with strong historical, political, and linguistic ties…
This work [i.e., the paper] follows a narrative structure focusing on the meso-level and macro-level of the Narrative Policy Framework (NPC), i.e., on ‘how policy actors construct and communicate narratives to influence the policy process’; and ‘how policy narratives permeate institutions, society, and cultural norms’ (Shanahan et al., 2018). This non-experimental design (case-study) evaluates the different characters in the COVID-19 handling in Sweden, with the Public Health Agency as key player. The setting for the meso-level assessment is Sweden during 2020, mainly focusing on the national level, although regional and municipality levels are discussed when relevant.
I’ve got to interrupt this ‘flow’ here for a moment to comment on what the authors are doing: contrary to their above introductory claim (no. 9), they actually do advance social science theory, in particular ‘NPC’ (on which see here and here, and of course, NPF has its own dedicated online presence).
As I’ve held above, this is what under more ‘normal’ circumstances would qualify as ‘Great Man Theory’, and I don’t know as to why the authors wish to explore structures (such as public health authorities, their decision-making procedures, and policy implementation) by means of narratology, i.e., emails and media statements by key personnel. It’s an intellectual fallacy and a logical non-sequitur.
At least the authors are honest (enough) about the nature of their piece: a case-study, and since there’s no real mention so far of the possibility of arriving at wider implications of their findings, I suppose we may as well stop reading here.
We conducted a content analysis, based on extensive discussions among the co-authors and other national and international experts, a comprehensive systematic literature search of scientific peer-reviewed papers, governmental reports and communications, and mainstream media outlets and digital media. To also assess how macro-level narratives shaped public policy, we explored the pre-pandemic shared societal and cultural values present in Sweden.
So, whatever ‘a content analysis’ actually means may be ‘revealed’ by exploration of any of the linked NFP content above, I presume. It’s not stated here, but the second subclause is particularly revealing: this piece is ‘based on extensive discussions’ among the authors who also wrote a few emails to other ‘experts’. In other words—self-referentiality at its worst. Shall we also mention group-think and group bias as confounding variables (that, by the way, remain unaddressed in this section)? Instead, we get mumbo-jumbo like this:
We evaluated the Swedish COVID-19 policy based on the following four distinct intellectual tasks (Lasswell, 1971; Nachmias, 1979): (a) identification of goals to be achieved in policy implementation, (b) metrics which can be used to assess progress (or lack thereof) with respect to goals, (c) data or evidence [these are really the same, ain’t it?] related to such metrics: official COVID-19 statistics, reports from healthcare and others and, (d) judgments of responsibility for policy outcomes which might be useful in efforts to improve future performance, to incorporate policy learning into new contexts (Pielke and Boye, 2019). We applied a well-established logical framework of policy evaluation to the intellectual task of assessing the use (and misuse) of science in COVID-19 pandemic management in Sweden. By scientific evidence, in the context of this paper, we refer to the advice of international authorities in infection control (including the World Health Organisation, (European) Centres for Disease Control and Prevention), and the body of peer-reviewed scientific papers. We evaluate the use of scientific evidence in terms of ‘scientific integrity,’ defined as consisting ‘of proper reasoning processes and handling of evidence essential to doing science’ and ‘a respect for the underlying empirical basis of science’ (Douglas and Bour, 2014). We applied the logical structure of a policy evaluation to assess scientific integrity in four contexts: (1) the pandemic preparedness; (2) the evaluation of the different actors in the pandemic; (3) errors and inconsistencies in the recommendations and communications; and (4) the consequences on healthcare and society.
This is so bad I almost can’t go on. There’s no indication, and even less inclusion, of the fact that ‘the science’ never stops evolving—things do change over time, and in the case of 2020 and all matters Sars-Cov-2 and Covid-19, it did literally overnight.
Note, further, that the authors’ ‘we’ is used consistently according to the above-related ‘methodology’ of ‘extensive discussions among the co-authors’. The ‘definition’ of ‘scientific’ evidence boggles the mind, to say the least, in particular after the gigantic clusterfvck of the past two years of public health authorities’ and their performance.
Next, keep in mind that the authors state, in their introduction, that they cannot do a ‘comprehensive’ approach to the subject, but in this section, they claim the exact opposite.
Finally, and apart from the ‘we’ issue outlined above, whatever is ‘scientific integrity’? Yes, there’s a definition, but I object to it: ‘science’ isn’t a thing—it’s an outlook, or approach, to fulfil one’s intellectual curiosity. ‘Integrity’, on the other hand, is a character trait, i.e., the people who make up the structures of, say, public health authorities, may have ‘integrity’, but there’s no mention of these confounding variables.
All of the above must be said before we come up with the problems with the data that underly any of these issues. Sigh.
So, one last quote from this section:
All authors have lived in Sweden at least through part of the 2020–2021 pandemic and form a multi-disciplinary group with a background in epidemiology, medicine, religious studies, history, political science, and human rights. The group was advised by several national and international independent experts. Ethical approval and informed consents were not applicable since this article does not contain any studies with human participants performed by any of the authors.
Curiously enough, the authors’ internal discussions don’t qualify for pre-publication ‘ethical approval and informed consents’. Well, given the above issues, I suppose we may consider this piece ‘junk’ anyways, but this is beyond ridiculous.
Results Include (I’m not making this up, btw)…
The most prominent official actors in the pandemic are described in detail in Supplement 3, as well as how they operate and the Swedish crisis management structure. These include: the Swedish Government (including the Prime Minister) and Parliament; The Public Health Agency; The National Board of Health and Welfare; Statistics Sweden; The Swedish Civil Contingencies Agency; The Swedish National Agency for Education; The Swedish Association of Local Authorities and Regions; The Health and Social Care Inspectorate; The Swedish Work Environment Authority; and The Swedish Institute.
Geez, these ‘official actors’ must number in the hundreds, to say nothing about all the pencil-pushers involved in the supporting bureaucracy of the Swedish gov’t, Parliament, and the official bodies. I’m kinda glad this isn’t ‘a comprehensive’ survey… (/sarcasm)
For Perspective, we turn to Larry Romanoff
For a discussion of the ‘results’, we now turn to Larry Romanoff who’s done quite an apt job of synthesising the paper’s findings (I think all of these quoted passages may be highlighted, but then it wouldn’t make any sense, doesn’t it):
Sweden’s litany of sins in this regard is almost too long to list, but includes incompetence, reckless disregard for medical science, secrecy, lack of transparency, cover-ups, manipulation of data, destruction of evidence, euthanasia, shocking medical mistreatment, deliberate death sentences of the elderly and infirm, criminal malfeasance, and much more. These are in addition to the fact of a failed policy that appears to have been guided mostly by incompetence…
It seems that several years earlier the Swedish government delegated pandemic management to its Public Health Agency, and then dismissed almost all the staff. If you recall, this is precisely the path taken by the US when John Bolton eviscerated the only US pandemic agency. This left Sweden with its main health authority that “lacked competence and could ignore scientific facts”. The report stated, “The Public Health Agency did not base its advice on scientific evidence but on preconceptions about influenza pandemics and herd immunity, relying primarily on a small advisory group with a narrow disciplinary focus and too limited expertise.”…
The report stated further that this central body was “systematically incorrect in its risk assessments, and ignored scientific evidence”. As one indication, Anders Tegnell, the so-called epidemiologist who devised Sweden’s strategy to deal with the Covid-19 epidemic, stated firmly, “What we are doing works. With us, there is no lockdown and no second wave”, this while immediately heading into the second wave. Tegnell also “labeled the advice of national scientists and international authorities as “extreme positions”, causing the [Swedish] media and political bodies to accept [Tegnell’s] own policy instead.”…
In addition to questionable health decisions, the study highlights the Swedish authorities’ lack of transparency, and even speaks of “secrecy, cover-up and manipulation of data”. The report stated that the State Epidemiologist began automatically deleting any emails requested by journalists or others. One report stated, “Although this is illegal, the practice of withholding information and deleting emails has become widespread among [Swedish] official agencies during the pandemic leading to so-called “shadow management”, as apparently the risk of legal sanctions is very low for power holders.”
The report’s conclusions are an undefended (and indefensible) condemnation of Sweden’s policy that casts disturbing shadows over its government as well. According to the report, “This pandemic has revealed several structural problems in Swedish society, at the political and judicial level, in health, in the official media and in the bureaucracy, with decentralization, lack of accountability and independence, and the rejection of accurate and complete information to the public as recurring problems at different levels.”
What else is there to say?
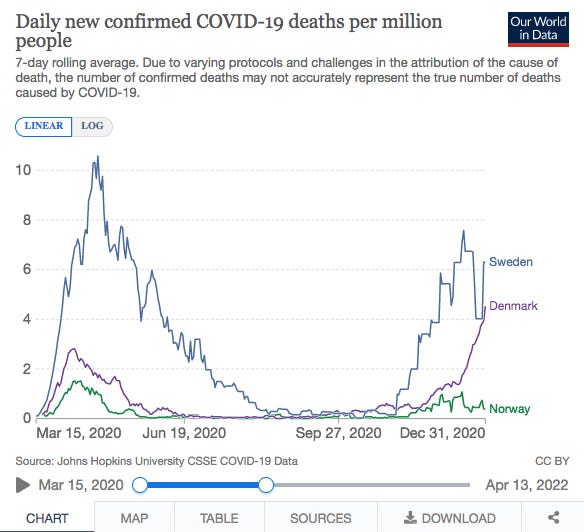
Outcomes, via OWID, of Covid-associated deaths during the paper’s study period:
Or, if you prefer numbers to-date, courtesy of Mr. Romanoff:

Do go ahead, read these pieces, get angry—and demand justice.
Did you send this article of yours to them?
I remember the libs are always quick to ask: "Are you a medical doctor?"
Are they?
This article is fraudulent in the extreme and I would not be surprised if one or two of the authors has ties to AstraZeneca. This especially is truth mixed with a great lie, and if the rest of it follows this the whole thing should be used for teaching how to dress up propaganda in academic rags:
"Many elderly people were administered morphine instead of oxygen despite available supplies, effectively ending their lives."
1, Sweden had up until mid nineties about 5 000 respirators ranging from simple oxygen masks to fully mechanical lungs, half of these belonged to the armed forces and were mothballed but kept fully operational. Mid nineties the socialist democrats in concertwith all other parties decide that there will never ever be a crisis or a war again and scrapped 99% of the resources created during the Cold War, including throwing away or selling abroad the mothballed equipment even though many agencies clamoured for being allowed to buy it (the civil defense and the firefighters were f.e. example forbidden to buy tracked vehicles and helicopters). This was to ensure that the backers of the moderate party would get to sell newish stuff to the armed forces and other authorities. Any lack of equipment is fully due to this time and these decisions.
2, The remaining respirators were placed under regional hospital administration, including units used in nursing home and old age residences meaning they were put in storage unless in emergencies oron doctor's direct orders. So a bureaucratic SNAFU is the real reason respirators weren't used, as this would further expose the political mismanagment.
3, Giving the old morphine instead of food, water or medical treatment is standard practice in many state run nursing homes, due to being chronically understaffed. It's far easier to take care of 20 elders if they are doped up on morphine after all.
Sadly, this is the level of swedish academia. This is not an outlier or anything unusual but rather middle of the road and typical.
The only real lingering problems created - and that has been fully created by governement decisions not infections - is that many people who were sacked due to closing of venues during 2020/2021 moved on to other jobs creating problems for many restauranteurs and similar, though that has largely been rectified thanks to the governement doing nothing, and that dentists and hospitals now have a backlog of patients to cope with on top of 25 years of neoliberal idiocy and greed. (Swedish health care uses NPM, and we have as of now more administrators and bureaucrats in public health care than doctors - it's not far off to say that we spend the most per capita in the EU, for the fewest doctor/patient hours, and with the fewest beds and lowest accessibility. We pay the most and get the least so to say.)
As for the death toll, the swedish municipality of Sölvesborg had the best result, due to the local councilor in charge basically asking the head of relevant departments: "What do you need from me to do your jobs and keep people from getting so sick they die?" The Florida aproach if you like. This is not acknowledged in any way in swedish media, due to one fact:
The party in charge in Sölvesborg is the Sweden Democrats. And US/EU media's Trump Derangement Syndrome has nothing on swedish media's anti-SD bias and outright outspoken hate. So since the "wrong party" happened to do right - schhh!
And 85% of those who died were over age70, in poor health, with comorbidities and/or were negro migrants (vitamin D, wrong food, stays indoors all winter and so on).
Henrik Wallin puts it much more succinctly than I can, but hopefully this helps explain some of the idiocy in that passel of lies you quoted.