


History Matters
An Excerpt of J. Henderson, ‘Fighting the Plague in Early Modern Italy’ (2020)

And now, dear readers, for something related, if quite different.
Since I teach history, I thought you may or may not—please peruse the comment section below to indicate assent or dissent—enjoy a bit of scholarly writing by colleagues who don’t know that I do this.
To kick off this (perhaps) multi-part series, here’s a brief part of John Henderson’s recent article ‘Fighting the Plague in Early Modern Italy’, Centaurus 62, no. 2 (2020): 263-74. Below is an extract, if you’d like to access the rest of the piece, follow the doi: https://doi.org/10.1111/1600-0498.12303. Note that for reasons fo convenience, I’ve omitted the references.
Henderson is a professor of Italian Renaissance History at Birkbeck College, University of London (see his official website and his academia profile). He’s also the author of the (un-) timely monograph Florence under Siege: Surviving Plague in an Early Modern City (Yale University Press, 2019), if you’d like to read it—it’s well worth it, but I also understand that you may not want to read about past epidemics these days.
So, here is John’s piece.
Abstract
This brief survey article examines the strategies to cope with plague in early modern Italy, often hailed at the time and by historians as the country that provided the model for public health policies in other parts of Europe and even formed the basis for policies in subsequent centuries. The study is organised according to three mains themes that are familiar today, containment, mitigation, quarantine, which also lay at the heart of plague strategies in early modern Europe. The starting point will be to determine which measures contemporaries believed were particularly efficacious, through the lens of their own understanding of disease. Then, by juxtaposing recent historical and demographic studies, I examine the application and effectiveness of public health measures in a country that was comprised of a series of larger and smaller states. In the process, I seek to raise wider questions about whether it was human intervention or non-human factors, in particular regional ecology, that determined the impact of plague in particular areas.
Mitigation
If the geographical pattern of the spread of plague in the 17th century suggests that cordons sanitaire may have worked in some cases, especially when authorities took advantage of the natural topographical features of a region, was this also true of the other elements of “mitigation” and “quarantine”? As the 1570 recommendations to the English Privy Council suggest, the main aim was to prevent the spread of plague. As today, governments conducted a campaign to trace Patient Zero, and, once he or she was discovered, to track their contacts, whom the authorities placed in quarantine until they recovered or died. In Florence in August 1630, the finger of blame was pointed at a chicken-dealer, who had had the misfortune to travel towards Bologna to sell his fowl at the beginning of the epidemic. After being refused entry to Florence, he died in Trespiano, a small village 5 miles to the north. Shortly afterwards, a dealer in cloth who was passing through became infected, and his symptoms developed on his return to his home in the city centre.
This story can be repeated over and again for different parts of Italy, and often the beginning of epidemics was blamed on certain sectors of society, such as foreigners or beggars. Then, as plague spread, a complex system of contact-tracing and reporting was put into effect, both officially, by local police and public health employees, and unofficially, through informal neighbourhood health watches, who were encouraged by financial inducements to report people who broke the decrees of health boards.
Regulations that were put into force included restricting the movement of the population within the city by setting curfews, closing schools, banning mass gatherings, and gradually increasing restrictions on food markets as the plague got worse. Many shops and taverns were closed and many occupations were stopped, particularly those associated with the sale of second-hand clothes, which were seen as harbouring the corrupt vapours of disease. As has been well documented, this led to a considerable number of people breaking the decrees of the health boards, leaving one to ask to what extent government measures were enforced, given that those cases that came to trial probably only represented a small proportion of actual events.
Another area that plague could be potentially spread was through public involvement in religious activities. Contemporaries faced a fundamental problem, for if all public religious activity was banned to prevent the spread of plague, it was feared that God would prolong the epidemic to punish citizens for their negligence. While churches were gradually closed as mortality increased, the clergy in some cities insisted on continuing with processions on public religious festivals, as in Milan and Venice during the 1575–1577 epidemic and in Naples in 1656. In other cities, such as Florence, processions were re-introduced as the situation improved, to express gratitude for the intervention of the Virgin Mary and patron saints.
Health authorities across Europe employed a large staff to cope with the impact of plague. These included male doctors and female “searchers of the dead” to identify the disease, and medical staff to treat the sick. Others were employed to carry the sick to quarantine centres and the dead to be buried, functions undertaken in many Italian cities by members of voluntary fraternities. In Venice, this task was undertaken by members of the Scuole Grandi, made famous by their substantial halls and churches decorated by celebrated painters such as Jacopo Tintoretto, and in Florence by the Archconfraternity of the Misericordia, which still runs the city's ambulance service.
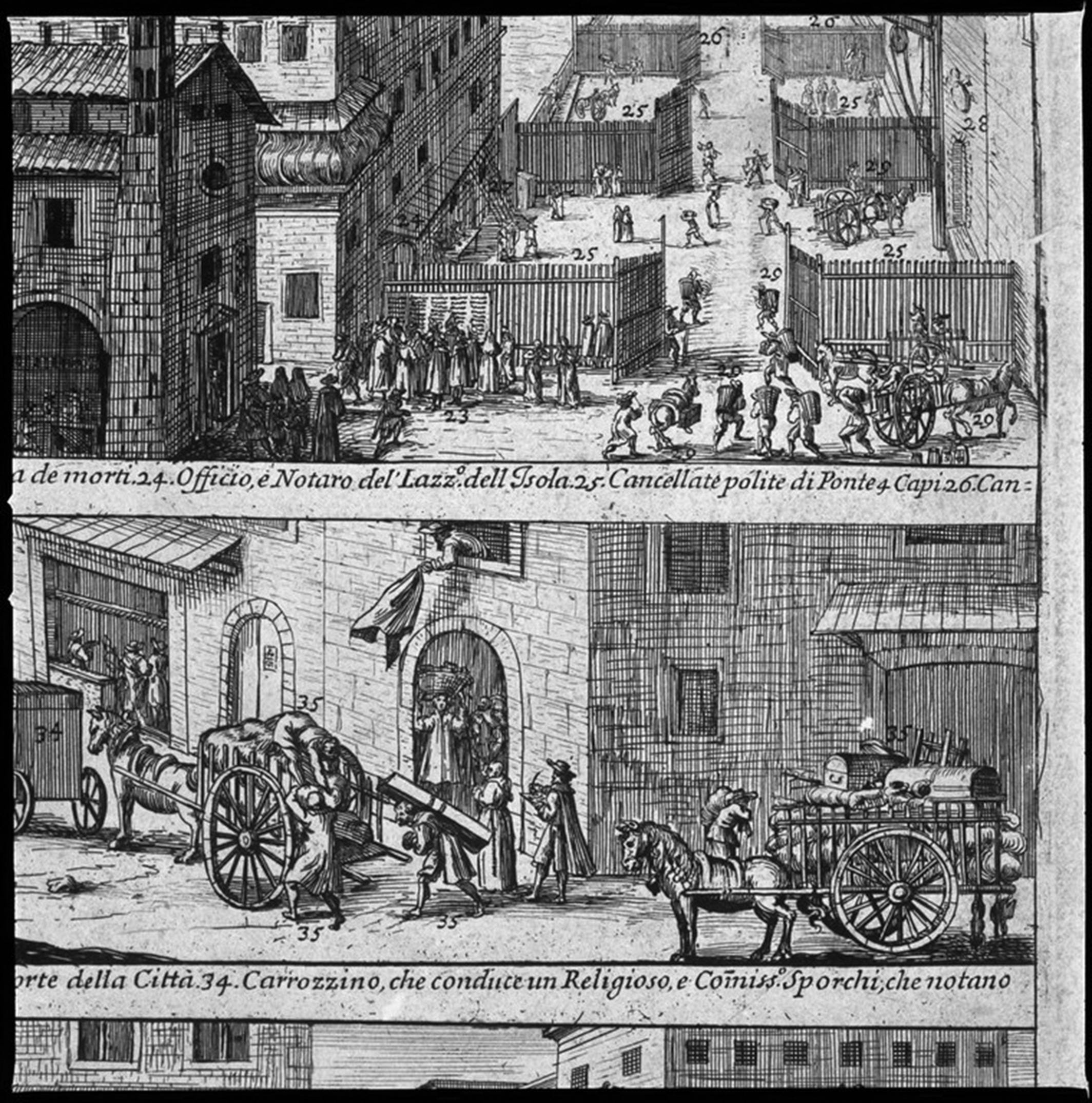
These initiatives represented very substantial investments on the part of Italian governments in terms of finance and personnel, and were justified by contemporary belief in their efficacy based on the understanding of the cause of the epidemic. The aim in disinfecting the houses and clothes of the sick and dead was to eliminate the fomites of plague, which were seen as sticking to material and objects. Fumigation of the possessions of a plague victim can be seen in the lower register of Louis Rouhier's etching (Figure 2). Health board employees vigorously throw out a range of household objects from the window of an infected house for their companions to fumigate or burn, since this was seen as one of the best ways to remove a major source and transmitter of infection. Not all people were treated alike, however, as can be seen in the bottom register of Figure 3, where a priest is shown leaving his locked-up house, while a note is made of his possessions to be taken away for fumigation. But it was not just infected objects that were removed from houses in Italy, but also sick individuals, who were taken off to be quarantined.
(Figures 2 and 3 are still linked to the original piece.)
Please let me know in the comments below if you enjoyed this (or not).
I enjoy a break from the daily “grind” of hearing about the abysmal behavior of elected and non-elected officials. Along these lines, I’ve been reading a book by Susan Humphries called “Dissolving Illusions.” Among other things, it discusses the public health response to smallpox since the 1800s. I’m amazed how things haven’t changed much. Forced vaccination, shaming of and restrictions on the unvaccinated, the failure of vaccines and vaccine harm, and the whitewashing of history.
“it was feared that God would prolong the epidemic to punish citizens for their negligence”—OMG, this sounds like Dr. Mengelfauci, today’s self-appointed God! 😆
I did indeed enjoy this piece, especially since I’ve always found the history of plagues fascinating and have listened to numerous audiobooks on the topic.