

Covid in Norway: October Update--pandemic of the seniors, 96-97% of whom are 'vaxxed', while everyone else is kinda o.k., 'irrespective of vaccination status'
Covid in Norway: October Update--pandemic of the seniors, 96-97% of whom are 'vaxxed', while everyone else is kinda o.k., 'irrespective of vaccination status'
An inquest into vaccination uptake and a bonus feature about media and public health gaslighting of the EMA's 'standard authorisation' of mRNA products

It’s been a while, I know, since we last talked about the ‘pandemic’ up here in Norway—and with good reason: most legacy media is extra-mum about virtually all matters Covid.
There’s but one small-ish ‘alternative’ outlet, document.no (h/t to Rikard), which briefly mentioned the recent ‘outcry’ generated by pieces that appeared in Die Welt and Politico around a month ago. I didn’t bother to bring this up, because there are many other places on the internet where these articles had been dissected. In addition, the piece over at document.no appeared on 9 Oct. 2022 only, i.e., some three-plus weeks after Die Welt and Politico published their pieces (which I consider a ‘limited hangout’).
So, what is ‘new’ over here in Norway with respect to Covid?
For background, please (re)visit my mid-September piece (content continues below):

According to the Institute of Public Health’s (IPH) best knowledge, the fourth injections were rolled out around week 40 (i.e., the first full week of October), and in my above-linked piece, I discussed all the relevant matters in great detail. Here’s a brief recap of the most important issues from that post:
like elsewhere, most notably in Austro-Covidistan, ‘infection’ does no longer count as ‘an epidemiological event’, i.e., what we’re witnessing here is the awesomely creative act of decoupling ‘infection with a pathogen’ from ‘injection of a product against…well, what exactly?’
The IPH admitted that whatever antibody response is elicited, it is—and always was—temporary (after a while, T cells and other mechanisms take over)…
Note that this renders measuring antibody numbers utterly useless, in particular as the Qatar study by Altarawhneh et al. (NEJM 2022, 387:21-34, doi: 10.1056/NEJMoa2203965) basically proves that injection with (presumably any) number of these mRNA products after infection doesn’t convey any lasting benefit to the vaccinee.
As I wrote back then, the IPH has formally entered cloud-cuckoo land; furthermore, the information peddled in mid-September is yet another shameful instance of dishonesty on part of public health officialdom.
Given the sad and sorry state of ‘reports’ by the IPH coming out (now only every two weeks, but without much useful data), there’s little to gain from presenting them to you. I’ve kept reading them, but there’s just not much to learn as most data has been scrubbed and the IPH is also mixing Sars-Cov-2 and Covid-19 with all other respiratory viruses.
On the one hand, this is perhaps what will eventually happen elsewhere, too, as the ‘pandemic’ loses its grip on the minds of most public health ‘experts’, ‘journalists’, and politicians…yet, the deplorable level of ‘information’ available to the general public is, well, a testament to the utter failure of public health authorities in one country.
If you’d like more proof of that, I’d invite you to venture over to the IPH’s dedicated website with the ‘self-declaration form’ any potential vaccinee is supposed to answer:
Nowhere would that form (I’ve linked to the English form, but here’s the Norwegian ‘original’) mention that the injectable products may be ‘problematic’ in terms of…
their ongoing phase III clinical trials (which will not end before late 2023);
the unprecedented number of adverse events (see here for the latest available report by the Nat’l Medicines Agency, or Legemiddelverket; the report is available in Norwegian ‘only’), but keep in mind that during this century’s first pandemic in 2009/10, the mass vaccination campaign was stopped after one (!) 8yo girl came down with narcolepsy—as of 20 Sept. 2022, there 265 dead in these reports that the NMA admitted to…)
or the fact that these injectables are experimental gene therapy.
Note, finally, that these forms were last updated on 8 April 2022, which is why I’d boldly claim that the recent decision by the European Medicines Agency (EMA) to confer ‘standard marketing authorisation’ status onto BNT162b2 (Comirnaty) by BioNTech/Pfizer and mRNA-1273 (Spikevax) on 3 Oct. 2022 hasn’t reached the IPH.
Hence, we may point to the fact that the IPH has been either misleading the general public about the experimental state of these injectable products since 27 Dec. 2020—or that the IPH is not doing its job properly in terms of providing accurate information.
I’d argue it’s actually both—at the same time.
It’s obvious that the IPH hasn’t been very honest about these products, their ‘safety’ (harm) profile, and the resultant impossibility of rendering informed consent.
It’s furthermore clear that the IPH continues to gaslight the public, as the absence of their efforts to stay on top of these developments shows.
Almost as an afterthought, mention shall also be made that these products—Comirnaty and Spikevax—are the only ones whose authorisation was ‘upgraded’ to ‘standard’. All other products remain in ‘limbo’, so to speak.
Furthermore, note that this applies to the ‘legacy’ version of both products; information about the ‘variant-specific’ booster injections can be found here.
To round this off, it suffices to note that these ‘details’ don’t seem particularly concerning to the IPH to warrant updating their website, the available materials, or the guidance to these products.
From the Surveillance Report for Weeks 39 and 40
There’s precious little that warrants attention: the report is full with boilerplate stuff and it can be accessed here. I’ll just share a few details here that are kind of relevant.
First up, who’s in the hospital? 4 out of 5 patients are seniors.
According to Table 3 (p. 7), the combined share of individuals aged 0-54 years is 11%; it’s very lopsided, and the majority of these 11% is actually in the 45-54 age bracket. There are some 9.9% who are in the 55-64yo bracket. In other words: in terms of severity of disease, Covid-19 is an old person’s illness, with 79.1% of all Covid-related hospitalisations occurring among those 65 and older. (All data valid for the past four weeks.)
The little information one gets in terms of ‘injection differentials’ is summarised on pp. 7-8 (my emphases):
Figure 2 shows the development in the incidence of the combination of hospitalisations with Covid-19 as the main cause of admission and Covid-19-associated deaths for people aged 18 and older. Fig. 2 also shows the number of vaccine doses the patients have received at least one week before the date of admission. The unvaccinated group are those who have not received any vaccine doses within a week before the date of admission. Due to the small population that has received only one vaccine dose (previously described as partially vaccinated), they are not included in the figure. In recent weeks, the incidence has been relatively stable in most groups, with some variation from week to week. The incidence is highest among people aged 75 and older, and in this age group it is highest among the unvaccinated. However, there are many important factors that must be taken into account in order to estimate vaccine effect, so the figures must be interpreted with caution.
And here’s the figure:
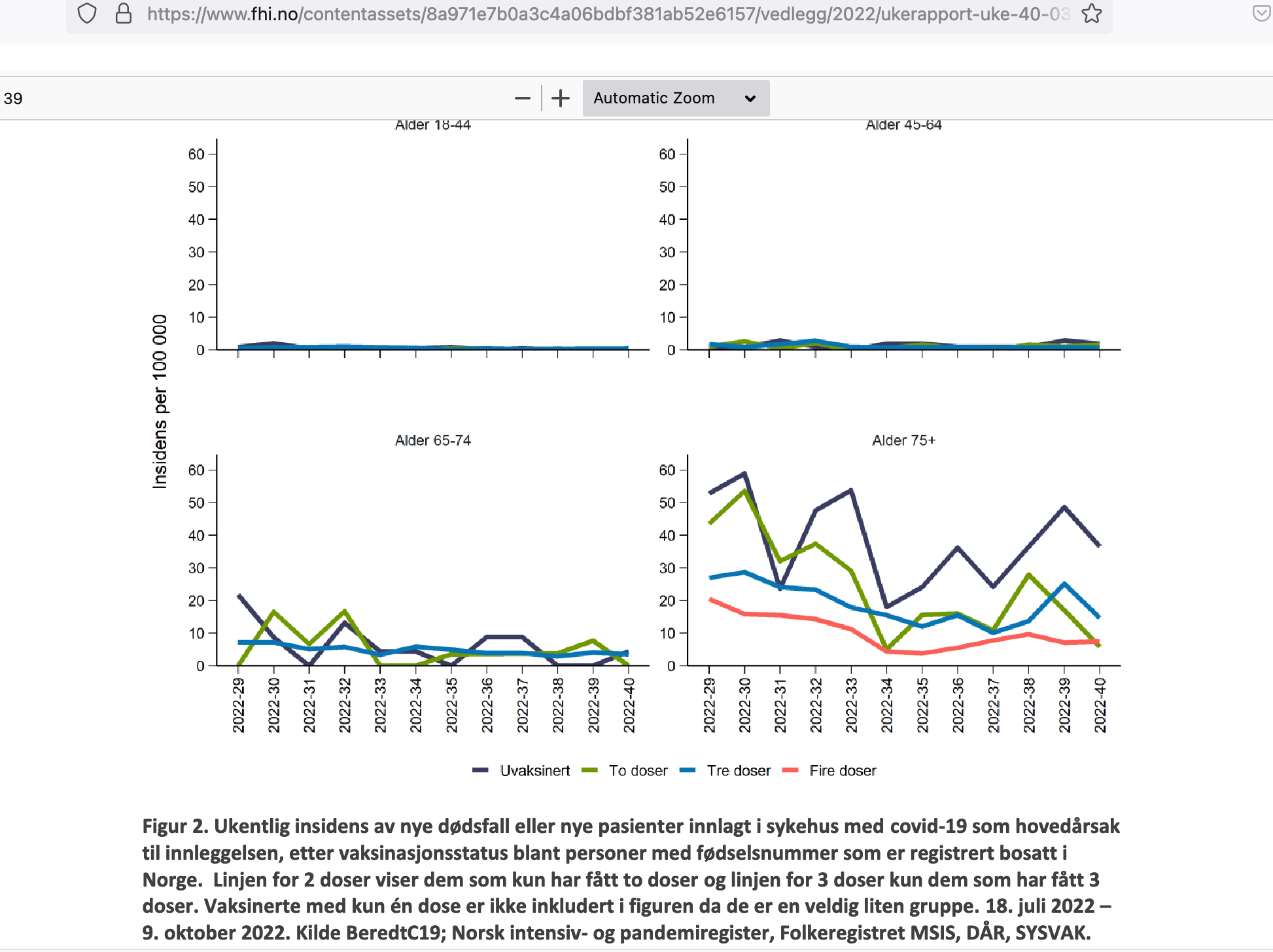
Note that there’s hardly a, if any, difference between ‘vaccinated’ and ‘unvaccinated’ incidences for those younger than 65.
Note further that the injection differentials for those older than 75 may be due to any (or a combination) of the following factoids: many seniors are already in a quite precarious condition, hence they may not have received any vaccine (and the exclusion of those who took one but no more doses may be relevant here). That’s also what to reasonably deduce from an enquiry into nursing home deaths in early 2021, which appeared in the Journal of the Norwegian Medical Association:
From a clinical perspective, it seems plausible that otherwise mild adverse effects from vaccination could potentially hasten death in particularly vulnerable patients and patients who were already in the final stages of life before vaccination. However, since the mortality rate in this group is very high anyway, a fatal outcome soon after vaccination may also be coincidental. It is important to assess whether there is a causal link between vaccination and death as this can help to guide the ongoing vaccination strategy.
I’m just curious about the exclusion of the one-dose recipients here, because their data might shed some light on these injection differentials…
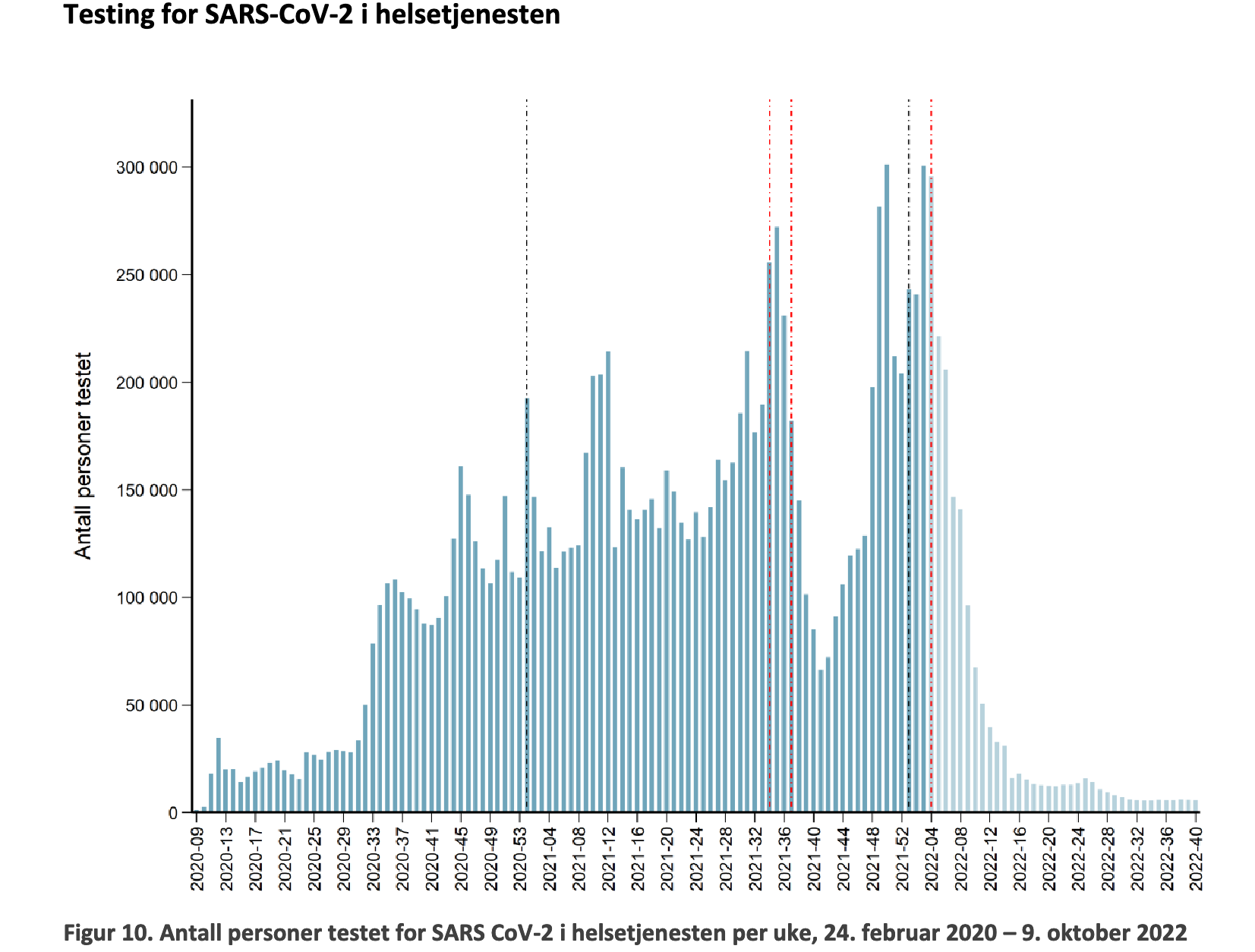
Moving on, we note in passing that testing for Sars-Cov-2 is basically close to nothing: since week 16 (2022), testing in healthcare settings has been lower than in spring 2020, and since August (around week 32), testing was curtailed even more:
Data from the ‘Sentinel’ surveillance also indicates that Rhinoviruses are a more pervasive issue right now, as shown in Fig. 19:

Finally, as per Table 10, here’s detailed data about injection uptake, as of 9 Oct. 2022:

Make of these numbers what you want, but I see no interest so far for increased booster-booster uptake, although that might change once the media gaslighting and ‘recommendations’ by the IPH are back in force.
As far as the above-mentioned issue of the exclusion of ‘partially vaccinated’ (one-dose recipients) is concerned, note the 96-97% uptake of the first dose among those 65 and older.
You may also revisit the above-reproduced age distribution and do your own ‘guessing’ as to the ‘vaccination status’ of the overwhelming majority of those hospitalised for Covid-19. Absent such data, we may probably assume that the ‘vaccination uptake’ shown here may translate into:
Hospitalisation occurs overwhelmingly among ‘the vaccinated’.
What do you think?
Due to niggling injuries and such I see a doctor semi-regularly (in Sweden you can supposedly "choose" a personal doctor from public health care - in reality you assigned the one who's available on the shortest notice; NPM in action), and from about February or so, they've gone quiet on Covid-vaccine.
No masking at the hospital, except when they actually should. Home tests on sale, stores removing plexi-glass shields, hand sanitizer in stores not being refilled or being removed completely.
Politically, Covid is about as relevant an issue as the Warsaw pact. Even the very varied mix of people opposing vaccines in general, medicine in general, science in general, and so on have gone back to their usual hobby horses:
Sugar causes all cancers, cereals destroys our digestion system, and keto [or rather, the current trend in miracle cures for obesity and everything from ahtlete's foot to pneumonia] is the one true way to eat - including for children under age one.
I think Norway will see the same development as you allude to an as we have had: Covid and the shots will be allowed to gently settle like something sinking to the bottom of the ocean. After all, Norway have real problems of their own, and I believe more and more norwegians are realising that they are set on the same path to national and ethnical suicide that we are, so the parties responsible will have to focus on keeping the lid on, at any cost.
One of the writers for Document.no is Helena Edlund; a swedish priest who is actually also a christian and as such has been the target of a smear-campaign from the swedish church, been the subject of harrassment by swedish taxation agents, andmuch more in the same vein. She is in my admittedly limited experience a woman of great conviction and principle, and I'd say here opinions and analysis is well worth considering no matter the topic.
I think the word therapy is at best misapplied. Why do genes need therapy?
Maybe these self-proclaimed injection concoction producing investors (just about all of you are invested methinks) are therapizing genetic codes for something other than for therapy. Or maybe they are simply clueless (about the long term genetics) morons wanting to make a quick government guaranteed buck, no matter to them how many people are harmed in the process. Oh, there is a word for that! Fascism.